The Relationship Between Diet and Osteoarthritis: Part 1

Osteoarthritis (OA) is the most common joint disease, affecting an estimated 10% of men and 18% of women over 60 years of age (Woolf et al., 2003). It´s pathogenesis involves diverse risk factors (such as age, biomechanical relationships, injuries and weight) affecting different tissues like the cartilage, subchondral bone, and synovium. Earlier on, OA was thought to be a “wear and tear” degenerative joint disease. However nowadays it is acknowledged that local and systemic inflammation play a key role in the disease progression and the emergence of pain.
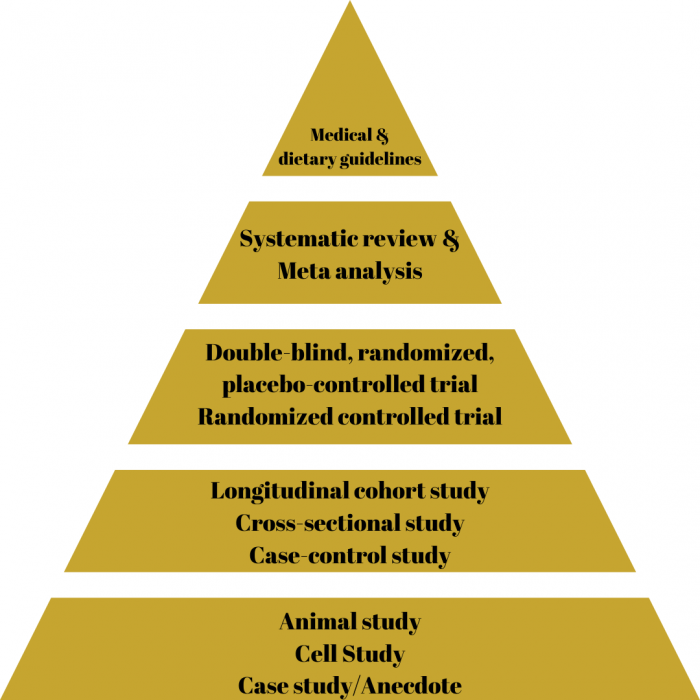
In the articles referenced in this blog, I will mostly name their study design because it is important to understand the hierarchy of evidence for a proper interpretation of the results (Murad et al., 2016). The hierarchy of evidence (as per the image below) portrays the idea that not all evidence is the same quality because some study designs are more prone to bias. While this hierarchy is a good way of thinking through results, especially in nutrition science one must know that certain areas of nutrition cannot be studied in a clinical trial and a well performed observational study might outperform a poorly controlled interventional trial. With interventional trials the quality of the evidence is also dependent on a randomization process, having a control group or even better a placebo group, while also blinding participants and researchers. With systematic reviews and meta-analysis far at the top of the evidence hierarchy, it is important to know that a meta-analysis can only synthesize the included studies and results are therefore only as good as the quality of the included studies.
OA impacts many areas of life and that’s why clinical assessment tools look at different aspects of the disease to portray a good picture of the disease in each person. Different assessment tools have been developed and validated.
| Name of Assessment Tool | What it Assesses |
| The Knee Injury and Osteoarthritis Outcome Score (KOOS) | Pain symptoms, activities of daily living, functioning in sports and leisure time, quality of life with the affected knee. |
| Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) | Pain, stiffness, physical function. |
| Japanese Knee Osteoarthritis Measure (JKOM) | Pain and stiffness, Conditions in daily life, general activities, health conditions. |
| Brief Pain Inventory (BPI) | Pain intensity, pain interference with activity interference (general activity and physical aspects of life) and affective interference (emotional or internal aspects of daily life). |
| Lequesne Index | Pain or discomfort, maximum distance walked, activities of daily living. |
| Visual Analog Scale (VAS) | Subjective measurement, in this case pain from 0 (no pain) to 10 (worst pain). |
| Short Form Health Survey (SF-36) | Vitality, physical functioning, bodily pain, general health perception, physical role functioning, emotional role functioning, social role functioning, mental health. |
Obesity and Osteoarthritis
A 2013 systematic review suggests a link between serum C-reactive protein and symptomatic rather than radiographic OA (Jin et al., 2015). This might explain why obesity is a risk factor for OA even in non-weight-bearing joints as excess visceral adipose tissue can lead to the release of pro-inflammatory adipokines (Yusuf et al., 2010; Azamar-Llamas et al., 2017; Jiang et al., 2016; Fan et al., 2020; Zhu et al., 2021). It has been shown that a decrease in body mass index units of two or more in patients with obesity will reduce the risk of developing OA in the next ten years by 54% while weight gain might slightly increase the risk for developing OA (Felson et al., 1992). Increasing BMI over a period of 10 years leads to a faster decline in tibial cartilage volume (Cai et al., 2019).
It has also been shown that patients with obesity can benefit from losing weight by a reduction in pain and systemic low-grade inflammation and that presence of joint damage does not hinder this reduction in pain (Gudbergsen et al., 2012; Richette et al., 2011). Weight loss improves OA disease severity in a dose dependent manner with 5% weight loss being good, 10% better and over 20% even better (Messier et al., 2018). Beside the metabolic benefit it has been shown that weight loss is associated with a reduced medial cartilage volume loss indicating an effect on the mechanistic-structural factors of OA (Teichtahl et al., 2015; Gersing et al., 2017). While finally obesity is a disease arising by an improper energy balance it also is a complex disease with multiple influences that are best treated with a multidisciplinary approach involving doctors, nutritionists and dietitians, psychologists, and other health care professionals.
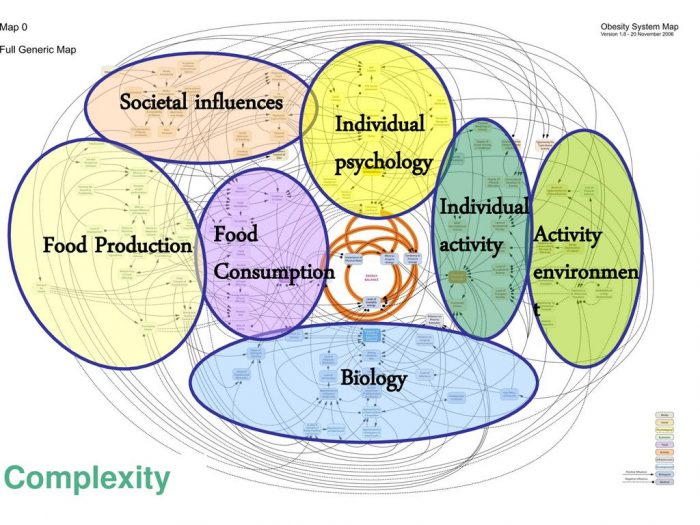
Blundell et al (2017)
The best a physiotherapist can do is to positively encourage his patients to look at the multiple treatment options, to stay away from weight stigma, and to perceive the complexity of the disease and not fall into the narrative of personal responsibility and lack of willpower (Grannel et al., 2021).
Nutrients and Osteoarthritis
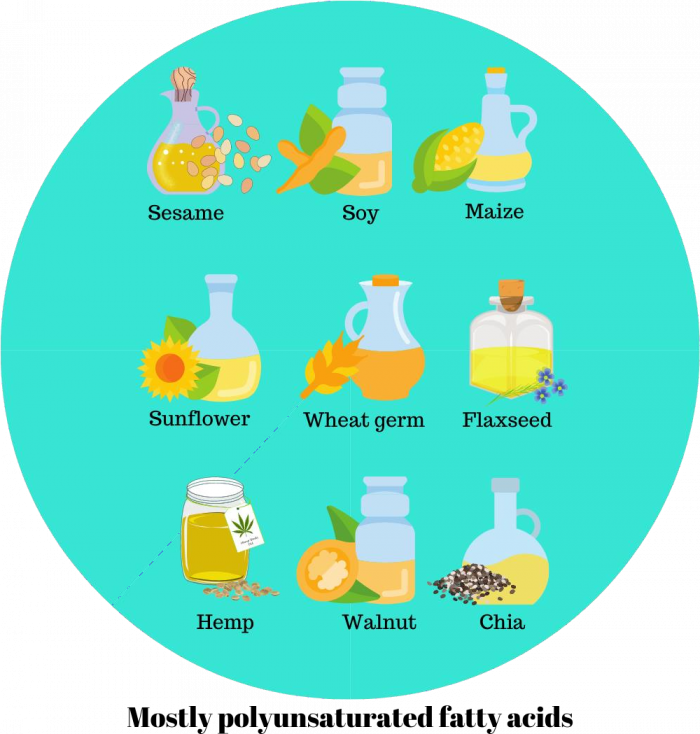
Fatty acids
In a longitudinal study with data from the OA initiative, patients with radiographic knee OA were followed up to 48 months while the dietary intake of fatty acids was assessed by food frequency questionnaire. Total fat and saturated fat intake showed a positive dose-response relationship with quantitatively assessed joint space width loss while the intake of polyunsaturated fatty acids showed an inverse relationship (Lu et al., 2018). With polyunsaturated fatty acids, especially the n-3 fatty acids in plasma showed an inverse relation with patellofemoral cartilage loss while the n-6 arachidonic acid in plasma showed a positive association with synovitis (Baker et al., 2012). In the MOST study, patients at risk of developing knee OA showed no association with plasma saturated, n-3 or n-6 fatty acid levels for developing radiographic or symptomatic OA (Felson et al., 2021).
Fish oil containing omega-3 fatty acids DHA, and EPA were also tested by four clinical trials. In one study patients received either 1000mg or 2000mg containing around 400mg of EPA and 200mg of DHA or nothing and had their knee pain measured by VAS scale, functioning tested by 100 meters walking velocity and three steps walking time which all improved compared to control and no notable differences between 1000mg and 2000mg (Peanpadungrat, 2015). In another double-blind trial patients with OA patients either received 15 ml pure fish oil or fish oil plus sunola oil containing either 2700mg of EPA and 1800mg of DHA or 270mg of EPA and 180mg of DHA (Hill et al., 2016). The primary endpoints were the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain score at 3,6,12 and 24 months plus changes in cartilage volume at 24 months. Secondary outcomes included WOMAC function, quality of life, analgesic and non-steroidal anti-inflammatory drug use and bone marrow lesion score.
Low dose fish oil had lower pain scores at 18 and 24 months with better functional limitation scores at 24 months while higher dose patients had better quality of life scores from 12 months onward. The use of paracetamol or NSAIDs, cartilage volume serum C-reactive protein was not influenced by treatment or time. In a trial with comparable design but different outcomes patients bone mineral density at the lumbar spine and femoral neck did not change after high and low dose fish oil supplementation (Chen et al., 2016). In the first placebo-controlled trial, patients received 2000mg DHA and 400mg EPA per day which reduced self- reported pain in patients with mixed OA after 16 weeks (Kuszewski et al., 2020). In another randomized clinical trial one group received 30ml of argan oil while the other group got no further treatment (Essouiri et al., 2017). Argan oil decreased pain as assessed by VAS scale and WOMAC pain index and further increased physical functioning and walking distance as measured by Lequesne index and walking perimeter.
Amino acids
Although alterations in amino acid metabolism have been proposed in OA, there is sparse evidence for a therapeutic effect of certain amino acids (Li et al., 2016). S-adenosylmethionine, a compound of the metabolism of the amino acid methionine has been researched in the 1980s with the last trial in 2009 (Kim et al. 2009). A meta-analysis from 2009 stated that the methodological quality of the studies is low and the effect small to negligible (Rutjes et al., 2009). Studies show no effect of L-Carnitine on CRP Values in women with knee OA (Malek et al., 2015; Malek et al., 2015; Baghban et al., 2021). 1000mg of L-Carnitine for 12 weeks also show no effect on hip circumference, visceral fat, fat free mass, fat mass, lipid profile, markers of oxidative stress, physical function and pain as measured by WOMAC score. Supplementing with HMB, L-arginine and L-Glutamine might lead to less loss of muscle mass after total knee arthroplasty in knee OA patients. 9g of essential amino acids after total knee arthroplasty also prevent rectus femoris muscle atrophy (Ueyama et al., 2020).
Fibre
Two cohort studies have looked at fibre – the Osteoarthritis Initiative and Framingham Offspring cohort. Fiber intake ranged from 9.1 to 21.9g in the Osteoarthritis Initiative and 14.1 to 26.6g per day in the Framingham study. The highest intake of fibre is associated with a dose-dependent inverse relationship with the risk of symptomatic OA. There also was a lowering in pain worsening for the highest quartile of cereal fibre intake which remained stable after adjusting for the lower BMI in the higher fibre group (Dai et al., 2017). No assosciation was found with incident OA. It is also worth noting that the higher fibre group also consumed less saturated fat, were more educated and consumed higher amounts of vitamin C and K for which all of them might exert their own influence on OA outcomes. In another analysis of the same studies BMI did mediate the relationship between fibre intake and symptomatic OA (Dai et al., 2018).
Vitamins A, C and E
Within cross sectional and longitudinal studies, several vitamins were examined and none showed a significant association with the incidence of OA, while a sufficient dietary intake of Vitamin C resulted in a 3-fold risk reduction for OA progression (McAlindon et al., 1996; Li et al., 2016). A higher dietary intake of Vitamin E and beta-carotene reduced the risk of OA progression. In a case-control study the serum alpha tocopherol levels in men were inversely correlated with the odds of radiographic knee OA while serum gamma-tocopherol levels were positively correlated suggesting a difference in tocopherol subfractions (Jordan et al., 2004). It has also been shown that normal levels of plasma vitamin C and E are associated with a protective influence for incident knee OA while high plasma values are associated with a higher risk (Chaganti et al., 2014; Seki et al., 2010; Wang). Short term supplementation with vitamin E shows symptom improvement in spondylosis, knee, and hip OA (Machtey & Ouaknine, 1978; Blankenhorn, 1986; Wluka et al., 2002; Brand et al., 2001; Scherak et al., 1990). Supplementing with 335g of Vitamin E (daily requirement around 12-15mg) did not influence the loss of medial and lateral tibial cartilage after two years (Wluka et al., 2002). The self-reported use of vitamin C supplements lead to a 11% risk reduction in developing knee OA while also having no influence on OA progression (Peregoy & Wilder, 2010). After two weeks of supplementation with 1000mg of vitamin C against placebo in patients with hip and knee OA pain measured via VAS was more reduced and physical functioning more enhanced as measured by Lequesne index (Jensen et al., 2003).
Vitamin K
A low dietary intake of vitamin K is associated with a higher risk of radiographic knee OA and narrower joint space width while not being associated with osteophytes area (Oka et al., 2009; Muraki et al., 2014; Misra et al., 2013). Decreased blood levels of vitamin K1 have been shown to be associated with a higher prevalence of OA, size of osteophytes and joint space narrowing in the knee and hand (Neogi et al., 2006; Oka et al., 2009; Neogi et al., 2006; ) They have also been associated with lower medial condyle cartilage thickness, an increased risk of radiological progression and higher disease severity in patients with knee OA (El-Brashy et al., 2016; Shea et al., 2015). Supplementing with 500μg of vitamin K1 (daily requirement around 60-70μg) for three years in a randomized controlled trial did lead to less joint space narrowing in only the participants with low baseline vitamin K1.
Vitamin D
As with vitamin C, a low intake of vitamin D is associated with a higher odds ratio of knee OA (Sanghi et al., 2015). Decreased serum vitamin D have been found in patients with knee OA (Heidari et al., 2011). Vitamin D deficiency was also found to be associated with an increased risk of developing and progressing OA in the hip and knee even if not all studies are showing this effect (Chaganti et al., 2010; Bergink et al., 2009; Felson et al., 2007; Zhang et al., 2014). Clinical trials trying to examine an effect of supplemental vitamin D have been inconsistent with either showing no or a small effect on the prevention of cartilage loss, the reduction of joint inflammation, pain, and physical function (McAlindon et al., 2013; Jin et al., 2016; Sanghi et al., 2013; Zheng et al., 2017; MacFarlane et al., 2020). 50.000 I.E.monthly for 24 months for maintaining serum vitamin D sufficiency led to an improvement in depressive symptoms in patients with knee OA as compared to placebo (Zheng et al., 2019).
Magnesium
Low serum levels of magnesium have been found in people with knee OA (Fincham et al., 1986; Hunter et al., 2003). A higher dietary magnesium intake is associated with a reduced odds ratio for radiographic knee OA, reduced pain and better functional outcomes and better knee cartilage architecture (Zeng et al., 2015 Qin et al., 2012; Shmagel et al., 2018; Veronese et al., 2019). A higher dietary magnesium intake is also protective regarding osteoporotic fractures in women with a high risk for knee OA (Veronese et al., 2017)
Selenium
There is no difference in the synovial fluid selenium concentration between healthy subjects and subjects with OA, which is also the case for copper, zinc, and iron (Yazar et al., 2005; Li et al., 2016). Selenium combined with the vitamin A,C and E did not show improvements in VAS scores for pain, stiffness or radiographic assessments after 6 months compared to placebo (Hill & Bird, 1990).
Antioxidant micronutrients
The dietary antioxidants lutein, zeaxanthin and β-cryptoxanthin are associated with a decreased tibial plateau bone area and decreased risk of cartilage defects (Wang et al., 2007; Wang et al. 2016). High serum levels of lutein and β-cryptoxanthin were also associated with a reduced odds radio for knee OA while people with high serum trans-beta carotene and zeaxanthin were more likely to have OA (Roos et al., 2001).
Polyphenols
Polyphenols are a class of phytonutrients of plants with high antioxidant properties that are not considered essential nutrients for life, but may be classified as healthy lifespan essentials. Four classes of polyphenols contain flavonoids, phenolic acids, stilbenes and lignans while flavonoids can be separated to flavanols, flavanones, flavones, flavonols, isoflavones and anthocyanins. Only some polyphenols to date have been tested in clinical trials regarding their effectiveness in treating OA. Pycnogenol is a standardized mixture extract of polyphenols from the French maritime pine. 50mg of Pycnogenol, three times daily, improved pain, stiffness, and physical function in patients with knee OA (Belcaro et al., 2008; Farid et al., 2007; Cisár et al., 2008). Plasma C-reactive protein and fibrinogen were also reduced. Flavocoxid, a product of two flavonoid, baicalin and catechins was deemed as effective as naproxen in improving OA symptoms (Levy et al., 2009; Levy et al., 2010). Turmeric extracts were shown to be effective against placebo in reducing OA pain and increasing physical function with similar results compared to NSAIDs despite not influencing inflammatory biomarkers like TNF- α, TNF- β, IL-6 and C-reactive Protein (Wang et al., 2021). Adverse effects were similar. What makes these results hard to interpret is the fact that different products with different dosages and curcuminoids were used, so the optimal turmeric product and dosage remain elusive at this point. Research for other polyphenols remains preliminary as it has only been done in cell or animal models (Valsamidou et al., 2021).
Supplements and Osteoarthritis
There are numerous supplements marketed for relieving OA symptoms, while only some already have clinical trials testing their effectiveness in humans.
Bromelain
One study with mild to moderate knee OA shows no superiority of 800mg against placebo while another study in moderate to severe knee OA shows equality of 500mg with diclofenac pain medication (Brien et al., 2006; Kasemsuk et al., 2016)
Glucosamine & Chondroitine
A 2018 meta-analysis found a reduction in VAS pain scores with either glucosamine or chondroitin supplementation, but not with a combination of both in patients with knee and hip OA (Simental-Mendía et al., 2018). WOMAC score indices for pain, stiffness and physical function were not affected by supplementation with glucosamine or glucosamine plus chondroitin sulphate. A 2021 meta-analysis found minimally improved joint structure and function while also minimally improving pain against placebo (Yang et al., 2021). Glucosamine and Chondroitin did not change the need for joint replacement. The trials mainly used dosages of 800mg to 1200mg of chondroitin and 1500mg of glucosamine.
Hyaluronic Acid
Oral hyaluronic acid alone as a supplement has been tested with a dosage of 200mg in patients with knee OA. After 12 weeks the symptoms as measured by the Japanese Knee Osteoarthritis Measure (JKOM) did not improve more than in the placebo group (Tashiro et al., 2012). However, it might be possible that hyaluronic acid works better in patients with severe pain (Sato et al., 2009).
Willow Bark
While a two-week randomized double-blind placebo-controlled trial showed a positive outcome regarding the WOMAC pain and VAS score in patients with knee and hip OA, no effect was shown compared to placebo or a control group and an inferior effect compared with diclofenac in a trial lasting six weeks (Beer & Wegener, 2008; Biegert et al., 2004; Schmid et al., 2001).
Collagen
A 2019 meta-analysis of six randomized placebo-controlled trials showed a positive effect of supplementing with mostly 10g of collagen hydrolysate or peptides in patients with knee or hip OA for WOMAC total, pain, stiffness and physical function and VAS scores (García-Coronado et al., 2019).
Probiotics
6×10⁹ Lactobacillus casei Shirota two times per day for 6 months were tested against placebo. WOMAC total, pain, stiffness, physical function and VAS pain score improved compared with placebo while also reducing serum C-reactive protein (Lei et al., 2017). In another trial with 5×10⁸ of Streptococcus thermophilus once per day for 3 month compared to placebo no change in WOMAC pain, function and stiffness scores or C-reactive protein was found despite an improvement in a cartilage breakdown biomarker (Lyu et al., 2020).
Creatine
A 2005 study showed that 10g of creatine per day for 10 days prior to total knee arthroplasty and 5g per day for 30 days after surgery did not prevent strength decreases compared to placebo (Roy et al., 2005). Creatine in combination with a lower limb resistance training program showed enhanced improvement in physical functioning, joint stiffness, lower limb lean mass and quality of life, while showing similar effects in pain reduction and no further effect on strength development (Neves Jr et al., 2011). Creatine also shows no effect on inflammatory or markers of cartilage degeneration or other disease outcomes after 12 weeks and did not prevent strength losses (Cornish et al., 2018).
Avocado/soybean unsaponifiables
Avocado/soybean unsaponifiables were first tested 1997 and showed effectiveness in a randomized, double blind, placebo-controlled trial in patients with knee and hip OA. Five other studies have been done and show that 300mg to 600mg are superior to placebo in terms of reducing NSAIDs usage and pain, improving functional disability and preventing further joint space width loss in some individuals with knee, hip, or temporomandibular joint OA (Blotman et al., 1997; Maheu et al., 1998; Appelboom et al., 2001; Lequesne et al., 2002; Maheu et al., 2014; Catunda et al., 2016).
Freeze dried aqueous olive fraction
In a randomized double-blind placebo-controlled trial patients with OA received capsules with 400mg freeze dried aqueous olive fraction or placebo (Bitler et al., 2007). Physical functioning, joint tenderness and inflammation were tested with the quality-of-life questionnaires. Physical functioning and disease activity improved more in the intervention group of patients with OA. Physician´s assessment of disease, profile of moods state and Matrix metalloproteinase 2 (MMP-2) did not change.
Artemisia annua
150mg and 300mg Artemisia annua have been tested for 12 weeks against placebo for improving WOMAC and VAS score in patients with hip or knee OA. 150mg showed improvements in WOMAC total, stiffness and physical function and VAS pain score (Stebbings et al., 2016).
Andrographis paniculata
300mg and 600mg of dried Andrographis paniculate extract were tested against placebo in patients with knee OA. WOMAC total, stiffness, pain, and physical function score as well as fatigue scores and quality of life improved equally compared with placebo (Hancke et al., 2019).
Boswellia serrata
338mg of Boswellia serrata extract has been tested in a double-blind, placebo-controlled trial for 3 months in patients with knee OA showing a decreased WOMAC total score, meaning an improvement in pain and stiffness while also enhancing physical functioning. Pain as measured in other scales, ability to walk, quality of life and radiological assessment of joint width and C- reactive protein also improved (Majeed et al., 2019). This confirms the findings of a former trial with 999mg Boswellia serrata extract (Kimmatkar et al., 2003).
Elaeagnus angustifolia
600mg of Elaeagnus angustifolia extract has been tested in one randomized double-blind controlled trial against ibuprofen for pain severity and Lequesne Index showing equality with 1200mg of ibuprofen (Karimifar et al., 2017). In another study its whole fruit and medulla powder has been tested against placebo in patients with knee OA showing significant reductions in pain and improvement in physical function with the medulla powder against placebo while not improving any other scores with whole fruit powder. Joint crepitus, instability and swelling did not change between the intervention and placebo group (Ebrahimi et al., 2014).
Green-lipped mussel
Different green-lipped mussel extracts have been tested and while two of the studies lack a control group and blinding and another study only tested against fish oil without blinding another study tested against a placebo in a double-blind placebo-controlled manner in patients with moderate to severe hip and knee OA. While the three former studies show positive outcomes in WOMAC and VAS score and Lequesne Index the latter study with better methodology showed no difference in VAS or WOMAC pain subscale or quality of life. The extract instead showed an improvement in joint stiffness and paracetamol usage (Cho et al., 2003; Coulson et al., 2012; Zawadzki et al., 2013; Stebbings et al., 2017).
MSM (Methylsulfonylmethan)
In a randomized, double blind, placebo-controlled trial 3750mg of MSM were tested for 12 weeks in patients with knee OA. WOMAC and VAS score, Aggregated Locomotor Function test and SF-36 Quality of life questionnaire were used to determine efficiency. There were no differences in WOMAC total, pain and stiffness score, quality of life or physical function while a small improvement in VAS score was found (Debbi et al., 2011).
Wobenzyme
28 capsules of wobenzyme per day has been tested against 100mg diclofenac in a double-blind trial in patients suffering from knee OA (Singer et al., 1996). Pain at rest, in motion, walking, at night and pain tenderness improved similarly in both groups. A newer randomized, double- blind, placebo-controlled trial compared 6 tablets of wobenzyme, 150mg diclofenac and placebo for 12 weeks using the WOMAC and Lequesne Index (Bolten et al., 2015). Knee joint function and joint-associated pain improved in both the wobenzyme, and diclofenac compared to placebo while no difference was found between the treatment groups in the WOMAC index with a trend for better improvement in the diclofenac group.
Water-Soluble Chicken Eggshell Membrane
A 2009 randomized, double-blind, placebo-controlled trial with 500mg eggshell membrane was tested in patients with knee OA. The supplement showed a significant improvement in pain and stiffness, but not function and overall WOMAC score after 8 weeks (Ruf et al., 2009). In a comparable design with 450mg of eggshell membrane hydrolysate showed no difference in total WOMAC, pain, stiffness and physical function subscale, knee range of motion while improving individual 6-meter walking test results (Hewlings et al., 2019).
Deer Bone extract
In a randomized, double-blind, placebo-controlled trial patients with knee OA were assigned to getting either 550mg of deer bone extract or placebo for 12 weeks (Shin et al., 2018). There were no changes in VAS or WOMAC score assessments, blood inflammatory or urinary markers of OA progression compared to placebo.
👩⚕️ Want an easier way to develop your assessment & treatment skills?
🙌 Our Practical video sessions are the perfect solution!
🎥 They allow you to see exactly how top experts assess and treat specific conditions.
💪 So you can become a better clinician, faster.

References
Don’t forget to share this blog!
Leave a comment (1)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Hi, I’m just wondering where can I find the complete reference list for this blog? (The reference list on the webpage is not completed)