
A recent viewpoint paper set out to discuss the use and value of manual therapy, and whether it truly can be classed as ‘passive’ considering how it’s used in a clinical setting.
We reviewed this paper in the latest issue of our Research Reviews – where industry experts break down the most recent and clinically relevant studies, for immediate application in the clinic.
What you’ll read below is a snippet from the review.
Like the sound of these Research Reviews? – Learn more HERE
Back to the paper!
STUDY TITLE: Manual therapy: always a passive treatment? – Rhon and Deyle (2021)
Study reviewed by Robin Kerr in the September 2021 issue of the Research Reviews
Key points from the study
- Passive and active strategies can synergistically form a multi-modal treatment model.
- Separating manual therapy and exercise in research fails to capture real life clinical scenarios.
Background and Objective
Manual therapy has become a polarizing component of physiotherapy practice, with opponents arguing that passive therapies provide expensive and low value care. The authors of this viewpoint paper contest that this perspective is “shallow and overly simplistic”.
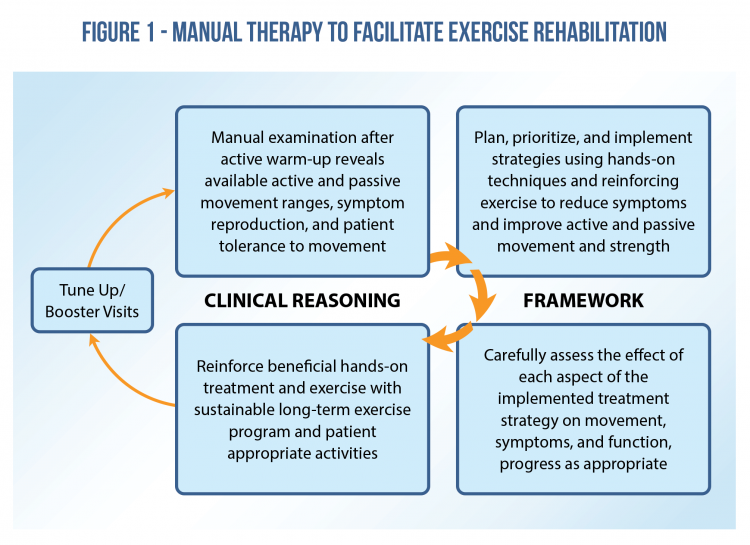
Taken in the context of how manual therapy is usually employed in the clinical setting, they propose that manual therapy is an integrated multi-element, active and passive management model founded on clinical reasoning.
Defining “Passive Intervention”and “High Quality Manual Therapy”
The definition of manual therapy is varied and confusing. In clinical physiotherapy settings, “passive” describes treatments such as modalities (e.g. ultrasound, electrical stimulation) and some forms of non-interactive manual therapy. It is this passive nature that points towards low value care.
The authors argue that high quality manual therapy has active participation of the patient to “reinforce, use, and perpetuate any changes in symptoms or movement that came about from the hands-on treatment”.
Implications for Synthesizing Research Results and Application
In many systematic reviews, manual therapy with active and passive components is often separated in an attempt to assess the isolated effects of manual therapy. The authors argue that in clinical practice therapists predominantly use a combination of manual therapy with other components such as exercise. Separating these in systematic reviews excludes a critical synergy in the real-life practice of manual therapy and importantly raises concerns that bias in the results of meta-analysis may occur.
Confusing Messages Affect Real-World Practice
A recent study on knee OA in which manual therapy was successfully integrated highlights the challenge for clinicians. Just prior to this study being published the American College of Rheumatology published guidelines for management of knee OA in which they recommended against the use of manual therapy. In the recent study, exercise was used in combination with manual therapy, highlighting the clinically reasoned and synergistic application of active and passive strategies (i.e. exercise and joint/soft tissue mobilization).
From this study’s perspective the two cannot be separated – the goal being manual therapy improves the quality and performance of the exercise/movement.
Clinical Implications
Debate on manual therapy may generate significant dissonance for the well-rounded, up to date clinician. It is clear from the pain-related research that manual therapy has a small effect size when used in isolation (as do other modalities such as exercise), so any clinician practicing purely passive manual therapy needs urgent updating.
Fortunately, in daily clinical practice manual therapy is rarely used in isolation, with most physiotherapists employing active and passive strategies within a treatment session. It is interesting to ponder whether a shift away from the use of any manual therapy is in fact a retrograde step. A multi-modal model involving synergistic passive and active strategies is promoted as optimal by the authors of this paper, and research supports that manual therapy is efficacious when used in this way.

Here’s what this review looks like in our September issue.
Do you want to save time by not having to wade through endless piles of studies?
Let us do the hard work for you!
Every month we summarise 12 of the most recent and clinically relevant studies in physio, for instant application in the clinic.
Learn more about these Research Reviews HERE.
Here are the 11 other studies we’ve reviewed in our September issue just published:
- Upper Limb Neurodynamic Tests for Cervical Radiculopathy
- Exercise Interventions for Patellofemoral Pain
- Heavy Resistance Training for Muscle Strains
- Is Hip Morphology a Risk Factor for Hip Osteoarthritis?
- Carpometacarpal Joint Injuries
- Facilitating Self-Management of Chronic MSK Pain
- Structuring Injury Prevention Programs
- Diagnostic Accuracy of Provocation Tests for SIJ Pain
- Kinesiophobia and Return to Sport After Shoulder Surgery
- Resistance Band Exercise for Frail Older Adults
- Effectiveness of Common Orthopaedic Procedures
📚 Stay on the cutting edge of physio research!
📆 Every month our team of experts break down clinically relevant research into five-minute summaries that you can immediately apply in the clinic.
🙏🏻 Try our Research Reviews for free now for 7 days!

Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!