

“…something serious in the woodshed…” (Cyriax 1982)
As clinicians, we deal with diagnostic uncertainty every day and we seek to minimise the risk of missing or delaying diagnosis of a serious pathology. Inevitably, at some point we are likely to miss serious pathology because it masquerades as a musculoskeletal condition. There is no one diagnostic test or red flag that we can 100% rely on to help us (Almond et al. 2009). Our clinical decisions on whether a serious pathology is present or not is complex and goes beyond just a list of red flags.
Often errors in missing serious pathology are reported for two reasons. Firstly, not recognising the red flags associated with the serious pathology, and secondly, failure to consider it as a differential diagnosis (Pope and Edlow, 2012). Being reassured by colleagues including GPs, and seemingly more experienced clinicians, that no red flags are present is also a common cause for failing to recognise serious pathology. The fact that serious pathology in most cases evolves over time only tells us that it may not have been present at the time they were seen by a particular individual. Reassessing and re-evaluating the change in a patient’s presentation over time is therefore hugely important.
In a quest to validate the use of red flags in clinical practice researchers have attempted to establish their diagnostic accuracy (i.e. the ability of a red flag to predict the presence of a serious pathology). Diagnostic accuracy helps us to quantify the extent to which red flags may or may not be informative about the presence of pathology. However, establishing good diagnostic accuracy is not easy because designing a prospective diagnostic study is extremely difficult due to the low incidence of reported serious pathology and the scarcity of epidemiological data. Consider spinal infection for example, where the incidence is reported to be between 0.2-2.4 cases per 100,000 annually in western societies, making it virtually impossible to carry out prospective diagnostic studies (Henschke et al. 2009). This makes these studies challenging to conduct, and as a result may influence how findings are interpreted and translated into clinical practice.
The vast majority of red flags have poor diagnostic accuracy, and so are not informative on the presence or absence of pathology. Even when moderate diagnostic accuracy exists, we should not rely solely or act on this information alone. A good example of this is a past history of cancer where when present, increases the likelihood of metastatic bone disease (MBD) from approximately 0.5% to 7.1% (95% CI 3.1 to 15.5) (Deyo, 1986). Also of note is that clinically around 25% of patients diagnosed with MBD do not have a primary diagnosis, which means we cannot be reassured in the absence of a past history of cancer.
We need to be cautious on the interpretation of guidelines where red flags are included and particularly where acting on one particular red flag is recommended. This is problematic when you consider that most individuals presenting with back pain will have at least one red flag (Premkumar et al 2018).
It is neither sensible nor practical to act on one red flag and can result in subjecting patients to unnecessary and worrying investigations, and in some cases unnecessary surgery (Cook et al. 2018).
Combinations of red flags increasing the likelihood of pathology have been largely unexplored (Verhagen et a 2016). Naturally it would make sense that the probability of the presence of serious pathology increases when more than one red flag exists (Premkumar et al 2018).
In practice, most clinicians do not act on a single red flag, but rather use a complex number of clinical reasoning skills, gut feeling, and understanding of how a serious pathology may present to help build a picture that may suggest a possible serious pathology (Langridge et al, 2015; Langridge et al 2016). Work is currently underway looking at a combination of red flags which may help to reduce the number of important symptoms clinicians need to look out for when making clinical decisions (Premkumar et al 2018).
[banner-ab-testing]
Context is important and whilst this might sound obvious it is not always applied. Again, a good example of this is a past history of cancer where a clinician’s index of suspicion is automatically raised but sometimes is the only catalyst for further investigation. Understanding which primary cancers are more likely to metastasise to the spine is necessary, followed by knowing which patients are more likely to develop metastases and why (Finucane et al 2017).
If we consider the lack of research evidence surrounding red flags, as a clinician it is hard to translate it into something useful and meaningful. Red flags in clinical practice are helpful providing we accept the limitations that the current research offers. We do however need to consider a more pragmatic approach that will be more useful in clinical practice.
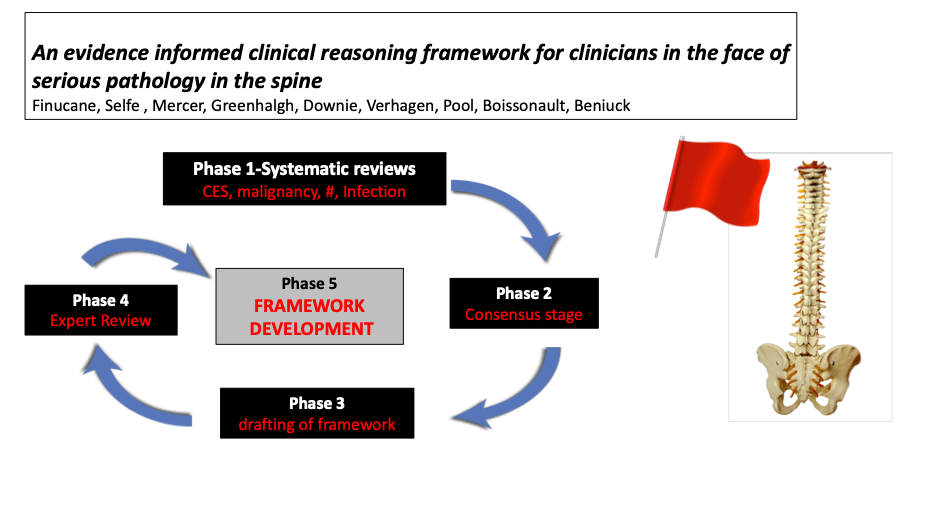
Research currently underway commissioned by the International Federation of Orthopaedic Manipulative Physiotherapists (IFOMPT) has committed to addressing the current position of the role of red flags in identifying serious pathology. It will focus on serious pathology of the spine, fracture, CES, infection and malignancy. The strength of this research is the utilisation of International experts from multi-professional backgrounds to gain consensus. The aim is to develop an evidence-informed clinical reasoning framework that will provide guidance to help clinicians reason their way through various potentially concerning spinal clinical presentations. The framework also aims to provide a clear reasoning pathway to help clarify the role of red flags in the management of these patients. It acknowledges, and builds on the role of red flags, but will also offer additional support for their continued use as part of a thorough and reasoned examination (Mercer et al. 2019). This approach is centred around the ability of a clinician to use strong clinical reasoning and careful questioning rather than rely solely on quantitative and experimental evidence, which we know to be limited.
It is hoped that this framework will be ready in time for the IFOMPT 2020 conference in Melbourne.
I would like to acknowledge in particular Sue Greenhalgh, Chris Mercer and James Selfe for the many discussions that have taken place over the years which has formed our thinking around the subject of serious pathology and hopefully added to the knowledge base in this area and will continue to do so.
Want to master behaviour change?
Dr Serena Simmons has done a Masterclass lecture series for us!
“Behaviour Change in Clinical Practice: A Physio’s Guide to Psychology”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!