From Research to Practice: Navigating Whiplash Recovery

No one talks about how tough it feels to have your life paused by a moment you barely remember… so let’s.
Three months after a road traffic accident, Avantika walked into my clinic with a stiffness that reached far beyond her neck. At 43, she was a busy working mother, a devoted morning walker, an occasional yogi, and someone who had always prided herself on being “independent and tough.”
But this injury? It was testing her in new ways.
The clinical setup: A story you’ll recognize
Avantika was driving home on a rainy evening when a motorbike slid in front of her car. She braked hard; the car behind her didn’t. The whiplash happened in seconds, her symptoms unfolded over days.
Now, three months later, she complained of:
- Persistent neck pain
- Headaches radiating from the base of her skull
- Shoulder tightness
- Poor sleep
- A rising fear of driving
She’d done her initial rounds of painkillers, rest, and one discouraging orthopedic visit where she was told, “It just takes time.” But time wasn’t helping. Functional tasks – long meetings, reading, household chores – were exhausting her. And it wasn’t just the pain. It was the uncertainty.
Subjective assessment: A puzzle with layers
Avantika described her pain as a combination of stiffness, “deep fatigue in the neck,” and intermittent sharp pain with rotation. She also reported difficulty concentrating, anxiety behind the wheel, and episodes of increased heart rate in traffic.
These symptoms flagged something beyond tissue injury, something the literature calls Whiplash Associated Disorder (WAD) II/III, where sensory, motor, and psychological factors interact.
She denied red flags such as:
- Sudden severe headache
- Visual disturbances
- Drop attacks
- Limb numbness or weakness
- Unexplained weight loss
- Night sweats
This cleared serious pathology (such as cervical arterial dysfunction), but her story hinted at central sensitization and psychological distress, both common in persistent WAD.
Her biggest fear? “What if this is my new normal?”
Objective assessment: What the body told us
Her examination painted a familiar picture:
- Reduced cervical ROM (especially rotation and extension)
- Painful cervical flexion-rotation test
- Weak deep cervical flexor endurance
- Overreliance on upper traps and sternocleidomastoid
- Local tenderness around C2–C4
- Altered kinaesthetic sense, slower, guarded movements
- Mild dizziness during head turns
- Slightly delayed muscle activation during arm elevation
Her posture wasn’t the problem, but her protective bracing certainly was.
Differentials I screened for included concussion, vestibular dysfunction, cervical radiculopathy, temporomandibular joint involvement, and thoracic outlet syndrome.
This was classic persistent WAD, but the prognosis remained good, especially with evidence-guided care.
Where research shaped the rehab plan
Three Physio Network’s Research Reviews played a major part in how I structured Avantika’s care. Each one offered a different lens: sensory-motor control, psychological interventions, and multimodal rehabilitation.
Let’s walk through them.
1. Exercise therapy for whiplash-associated disorders by Dr Julia Treleaven
This Review reinforced that persistent WAD is not “just a strained neck.” It is a nervous system issue, not only a tissue issue. It highlighted the importance of individualized care — WAD isn’t a single-pathway condition, and our exercise prescription must adapt to the person in front of us.
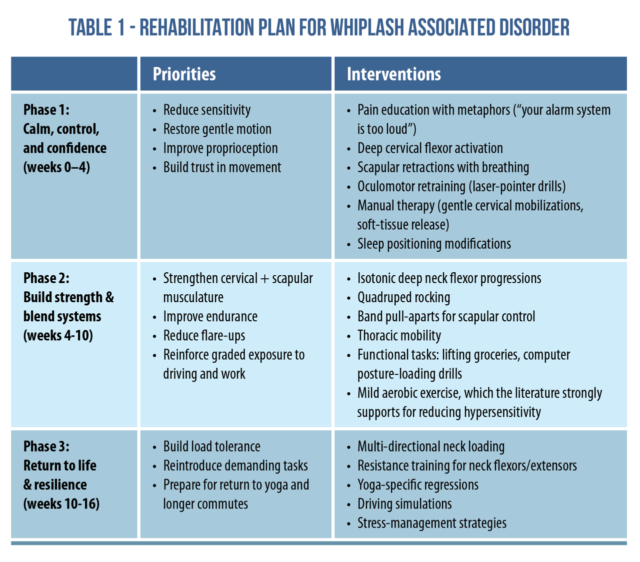
This formed the backbone of phase 1 of her rehab (see Table 1). The research helped me confidently explain that her dizziness, clumsiness, and reaction delays were normal, expected, and treatable. For Avantika, this alone reduced her fear significantly.
2. Effectiveness of psychological interventions for neck pain by Dr Sandy Hilton
This Review showed that CBT-based education, reassurance, and self-efficacy training significantly support recovery in persistent WAD.
Given Avantika’s anxiety, I integrated:
- Pain neuroscience education: reframing pain from “damage” to “sensitivity”
- Graded exposure to driving: starting with a parked car, then short drives, progressing to peak-hour traffic
- Self-efficacy support: using micro-wins such as maintaining neutral neck posture for 10 seconds or completing a Zoom call without pain escalation
She recorded all of her wins. Patients like Avantika often underestimate progress, so tracking this was transformative!
I also offered a referral to a CBT-trained clinician, should she wish to pursue more formal psychological support.
3. Traumatic neck pain by Dr Xiaoqi Chen
This Review gave clear direction on multimodal rehab for WAD:
- Manual therapy (graded, not aggressive)
- Exercise therapy
- Psychological input
- Patient education
- Vestibular and sensorimotor training
It also emphasized avoiding prolonged passive treatments and prioritizing active rehabilitation. This guided the entire structure of Avantika’s plan.
Turning research into practice: The rehab timeline
Even though she was three months post-accident, this was early rehab for her nervous system. See Table 1 for the three research-backed rehabilitation phases we progressed through.
And the results?
By week 4 she showed:
Improved head-turn accuracy, reduced dizziness, better sleep, and the ability to complete short drives without panic.
By week 10 she could:
Sit through a 90-minute meeting, drive 20–30 minutes comfortably, and hold deep neck flexor endurance for >30 seconds.
By week 16, she was 80–90% recovered and living normally – confident, pain-minimal, and functional.
Wrapping up
Whiplash isn’t just about the neck. It’s about physiology, psychology, and identity, all shaken at once.
Avantika reminded me:
- Patients don’t fear pain, they fear what pain means.
- Recovery is faster when we treat the nervous system, not just the muscles.
- Evidence isn’t optional, it’s the scaffolding of clinical confidence.
- People recover best when they feel heard, in control, and guided instead of guarded.
Her last line to me was:
“I wish someone had told me this wasn’t my fault, and that I wasn’t broken.”
That is why we do what we do.
Want to elevate your clinical decision-making for better outcomes? Subscribe to Physio Network’s Research Reviews – your shortcut to staying current, confident, and clinically sharp.
📚 Stay on the cutting edge of physio research!
📆 Every month our team of experts break down clinically relevant research into five-minute summaries that you can immediately apply in the clinic.
🙏🏻 Try our Research Reviews for free now for 7 days!

Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!