ACL Cross Bracing Protocol: Key Patient Selection Factors for Physios

The Cross Brace Protocol (CBP) is an emerging non operative management option for Anterior Cruciate Ligament (ACL) ruptures which involves placing the knee in a locked Range of Motion (ROM) brace for a certain duration of time to facilitate ligamentous healing.
As first contact clinicians it is important to understand how to identify someone who may be successful with the CBP. Understanding the patient selection criteria, injury characteristics, and practical considerations is essential for deciding whether to go down the CBP route. This blog outlines what to consider when deciding whether the CBP is a viable option for your patient.
If you want to see exactly how an expert manages a real patient through the CBP, check out Geoff Ford’s Case Study HERE.
What to listen for in the subjective
1 – Velocity
If the patient’s injury occurred at slow velocity then they are far more likely to meet the MRI criteria for success. Slow velocity incidents often result in an isolated tear of the ACL, without the concomitant injuries you see in high velocity incidents. For example, if someone has twisted their knee coming off a ski lift, they are much more likely to be eligible than someone involved in a high speed change of direction mechanism.
2 – Post injury function
Greater function immediately post injury with few adverse events (e.g., episodes of instability) is a good indicator for CBP eligibility. A patient may report that they were able to continue activities, or they may be able to complete a series of testing with no instability.
3 – Swelling
The patient may report that the knee did not swell immediately post injury. It is widely accepted that a large effusion is a classic sign of an ACL injury, but it is possible to have an ACL tear without immediate swelling. This is thought to be due to an intact synovial envelope, which wraps the ACL and supplies it with nutrients and blood. Therefore the fluid is not spilling out into the knee causing a large effusion. An intact synovial envelope enables continued supply of healing nutrients to the injured ACL, which is favourable for successful healing with the CBP (1).
4 – Time since injury
Patients should ideally be braced between days 4-10 post injury with a hard cut off at 21 days. The ACL should be considered the same as a fresh wound. When there is injury to the ligament, the same inflammatory sequence occurs. The clock is ticking to reduce the injured ACL tissues and re-locate the two ends close together to facilitate healing. After day 7, the cytokines drop off and continue to decline until the ACL has become involuted (closed over). If this occurs, it is too late to brace.
MRI factors
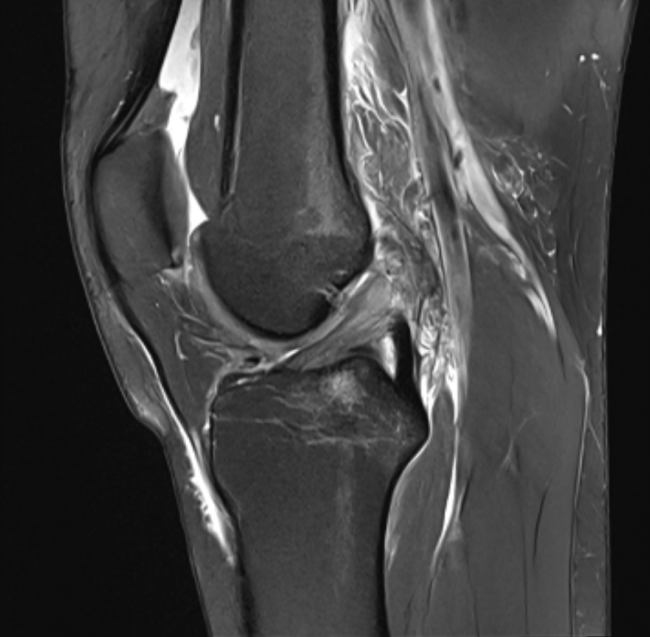
There are multiple factors to look out for on your patient’s MRI which may be associated with greater potential for healing (2), they include:
- Small gap distance (ideally less than 6mm between ends).
- Femoral origin still in tact.
- Tear in the proximal third of the ligament (1).
- Non displaced ACLs (fibres are in alignment and a large portion of the bundles have not flipped out of the intracondylar notch).
- Minimal joint effusion.
- Overlying synovial envelope intact (3).
These factors are all seen in the below MRI:
Patient-related factors to consider
This is an intense and difficult protocol. Yes, the injury meeting the anatomical criteria for success is one factor, but it is essential to look at the patient’s overall picture to determine if they are suitable. For example:
1 – Occupation
Patients working physically demanding professions may not be suitable candidates due to the strict non weight bearing requirements at the beginning of the timeline. However, individuals with a sedentary job will mostly be able to continue working unaffected, making them more suitable candidates.
2 – Home support
Patients who do best have a good support system in place to assist with daily life. Day-to-day activities such as grocery shopping and cooking become extremely difficult with strict ROM restrictions and crutches!
3 – Financial considerations
If a patient is worried about the financial costs associated with surgery, then CBP is considerably cheaper than surgical options. Patients who can not afford private treatment and have a long public wait ahead of them may wish to trial CBP in the meantime.
Myth busting
A common misconception is that young, active people with high functional demands require surgery and will not do well with conservative management for an ACL tear. This is not always the case.
The CBP should be an option to young, active people if they meet the criteria. It would be ill-informed to write off the CBP for a patient solely based on their age and activity demands.
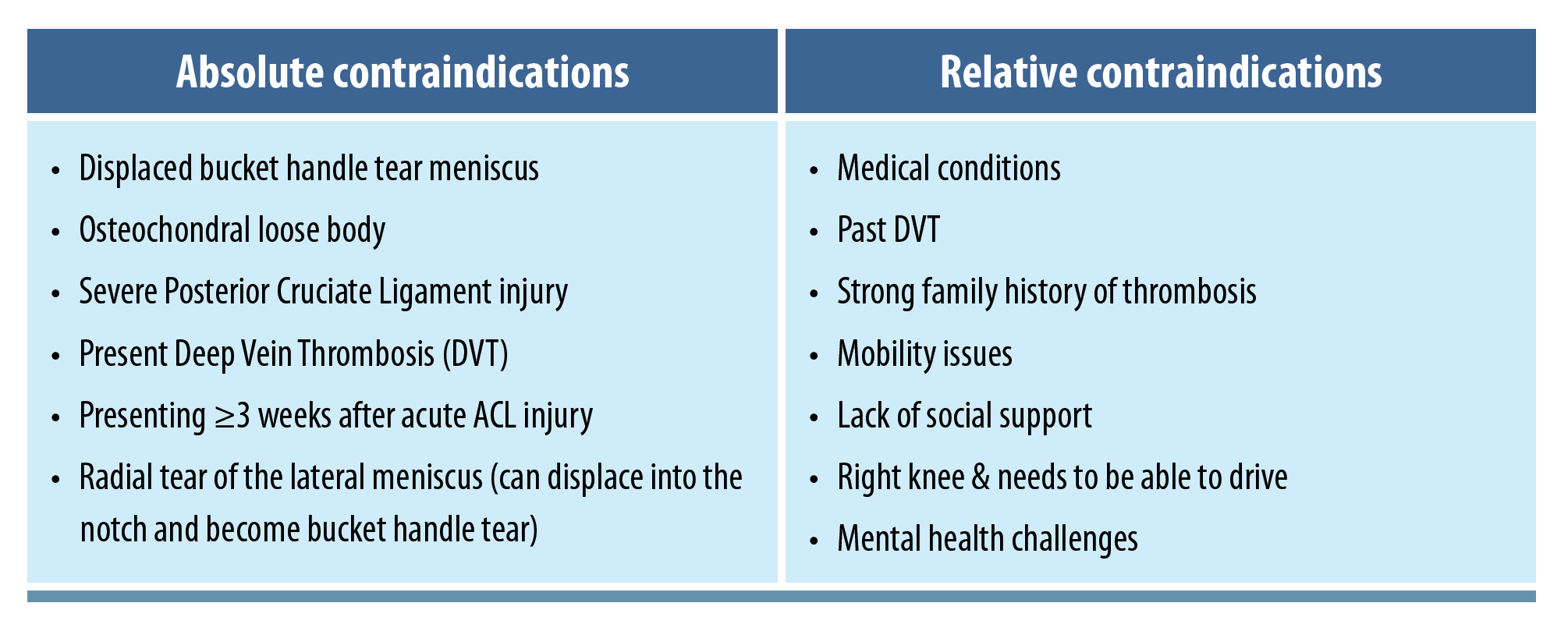
Additionally, if a patient doesn’t meet all criteria but is well informed and interested in trialling the CBP, they can still be offered a consultation. There have been cases of good outcomes for patients with flipped bundles that have spontaneously flipped back across the course of their bracing, or even patients who have braced close to the three week mark. See the table below for patient exclusion criteria to follow when considering the CBP.
What are the protocol options?
The original protocol had patients spending 12 weeks in a ROM brace. Given the protocol was a relatively new concept, this was chosen as a scientifically sound duration of time to allow tissue healing.
As the patient population grew, researchers realised that healing could be achieved within shorter durations. Thus was born the 8 week, 6 week and the modified hybrid protocol. Despite differing timeframes, the options each hail from the same principles. Selection of protocol duration is now dependent on the aforementioned patient factors, including severity of tear, concomitant injuries, and relevant medical and social history.

The 12 week protocol is now rarely prescribed, as the same success has been seen with the shorter protocols. Interestingly, researchers discovered those with a concomitant high grade Medial Collateral Ligament (MCL) injury could not be braced at 90-degrees for 4 weeks because they would get too stiff. This population is almost exclusively offered the 8 and 6 week options.
Wrapping up
The CBP offers a promising alternative to surgical management of ACL injuries for carefully selected patients, relying on early bracing to promote natural ligament healing.
Success depends on precise timing, MRI findings, and patient suitability across medical, occupational, and social factors. While not without its challenges, the CBP can provide excellent outcomes, even for some young, active individuals, when the criteria are met.
By understanding the mechanism of injury, post-injury presentation, and individual circumstances, clinicians can determine if the CBP is a viable pathway. With growing evidence and refined protocols, it presents an important option in the evolving landscape of ACL management.
If you want to know exactly how to manage your patients once they’re on the CBP path, watch Geoff Ford’s real life Case Study HERE.
👩⚕️ Looking to sharpen your clinical reasoning?
🙌 Our Case Studies service is here to help!
🎥 Watch case study presentations that reveal how top clinicians treat real patients…
🏆 And apply their strategies to get better results with yours!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!