From Research to Practice: Navigating Non-Specific Neck Pain

The strategies that feel safest when your neck hurts are often the very ones that keep the pain hanging around.
That was the uncomfortable realisation Elena came to during our second consultation.
Like many people with persistent neck pain, she had spent months trying to “protect” her neck. She avoided certain movements, kept her shoulders stiff during long work calls, and frequently stretched her neck throughout the day hoping it would loosen things up.
But paradoxically, those strategies were likely keeping her stuck.
This is the story of how Physio Network Research Reviews helped guide the rehabilitation of Elena, a 46-year-old head of sales and marketing navigating persistent non-specific neck pain in the middle of a high-pressure career.
Meeting Elena
Elena was the head of sales and marketing for a sports management company – a role which involved constant travel, long strategy meetings, and back-to-back Zoom calls with clients across time zones.
Her workdays often stretched to 10-12 hours.
She described her neck pain as a dull ache around the lower cervical region and upper trapezius, occasionally spreading toward the base of the skull. The pain had gradually developed over the previous eight months and had recently begun affecting her concentration during meetings.
Her main complaints were:
- Persistent neck stiffness, especially by late afternoon
- Headaches 2-3 times per week
- Difficulty turning her head fully while driving
- Fatigue in the neck and shoulders during long laptop sessions
Elena had tried massage therapy, occasional pain medication, ergonomic adjustments, and a variety of YouTube stretches. Some helped briefly. None created lasting change.
Her main goal was simple: “I just want to work without constantly thinking about my neck.”
Subjective assessment
During the subjective interview, a few important patterns emerged.
Her pain fluctuated but rarely dropped below a 3/10 and sometimes reached a 6/10 during stressful workdays. Symptoms worsened with prolonged desk work, long flights, and high-stress deadlines.
However, interestingly, she reported feeling better during her weekend tennis sessions and when she went for evening walks. This immediately raised a useful clinical insight: movement itself was not the problem.
Other key considerations included:
Red flags screened and ruled out:
- No trauma
- No neurological symptoms
- No unexplained weight loss
- No progressive neurological deficits
- No systemic disease indicator
Psychosocial factors:
- High occupational stress
- Long sedentary work hours
- Fear that “turning the neck too much might worsen things”
These psychosocial elements would later become an important part of the rehab process.
Objective assessment
The physical assessment painted a familiar picture seen in many people with persistent neck pain.
Findings included:
- Mild restriction in cervical rotation and extension
- Reduced endurance in deep cervical flexor testing
- Increased tone in upper trapezius and levator scapulae
- Scapular upward rotation slightly delayed during arm elevation
- Moderate discomfort during sustained cervical extension
Neurological screening was normal and importantly, there were no signs of serious structural pathology.
This confirmed what the clinical picture already suggested: non-specific chronic neck pain influenced by a combination of physical load, motor control, and stress factors.
Where the research came in
Three recent Physio Network Research Reviews helped refine the rehabilitation strategy and provide a clearer clinical direction.
Research Review #1: Deep Neck Muscle Exercises for Nonspecific Neck Pain
This Review by Dr Julia Treleaven, which helped shape Elena’s rehab plan, looked at the effectiveness of different exercise approaches for non-specific neck pain.
Interestingly, the Review reinforced something many clinicians notice in practice: most forms of exercise tend to help reduce neck pain, and no single approach consistently outperforms the others when pain relief alone is considered. However, it also highlighted that pain reduction doesn’t automatically mean neck function improves.
For patients like Elena, who had noticeable fatigue and reduced endurance in her cervical musculature, neck-specific exercises targeting deep cervical control were likely necessary to restore function, while broader strengthening and endurance work supported overall capacity.
The Review also reminded me to avoid chasing a single “best” exercise protocol and instead build a program around the patient’s presentation, goals, and beliefs, often combining exercise with manual therapy as part of a multimodal approach. In Elena’s case, this meant progressing from low-load cervical control exercises to more global neck and upper-back strengthening as her symptoms settled and her confidence in movement returned.
Research Review #2: Predictors of Persistent & Recurrent Neck Pain: Review
This Review focused on the psychological side of non-specific neck pain, particularly pain catastrophising and psychological distress.
Elena’s job as the head of sales and marketing meant long hours, constant deadlines, and a baseline level of stress that she openly acknowledged during the subjective assessment. The Review highlighted that factors like catastrophising and distress are strongly associated with persistent or recurrent neck pain, yet they are often under-screened in routine physiotherapy practice.
This prompted me to explore Elena’s beliefs about her pain more carefully; how worried she was about long-term damage, how much the pain affected her work confidence, and whether she felt in control of her symptoms.
Evidence suggests that approaches such as Cognitive Behavioural Therapy (CBT) and Acceptance and Commitment Therapy (ACT) can meaningfully reduce catastrophising and improve function when used within a multimodal approach.
While these interventions fall outside the scope of most physiotherapy sessions, the Review reinforced the importance of early screening and interdisciplinary collaboration, which led to an open conversation with Elena about psychological support options alongside her physical rehabilitation.
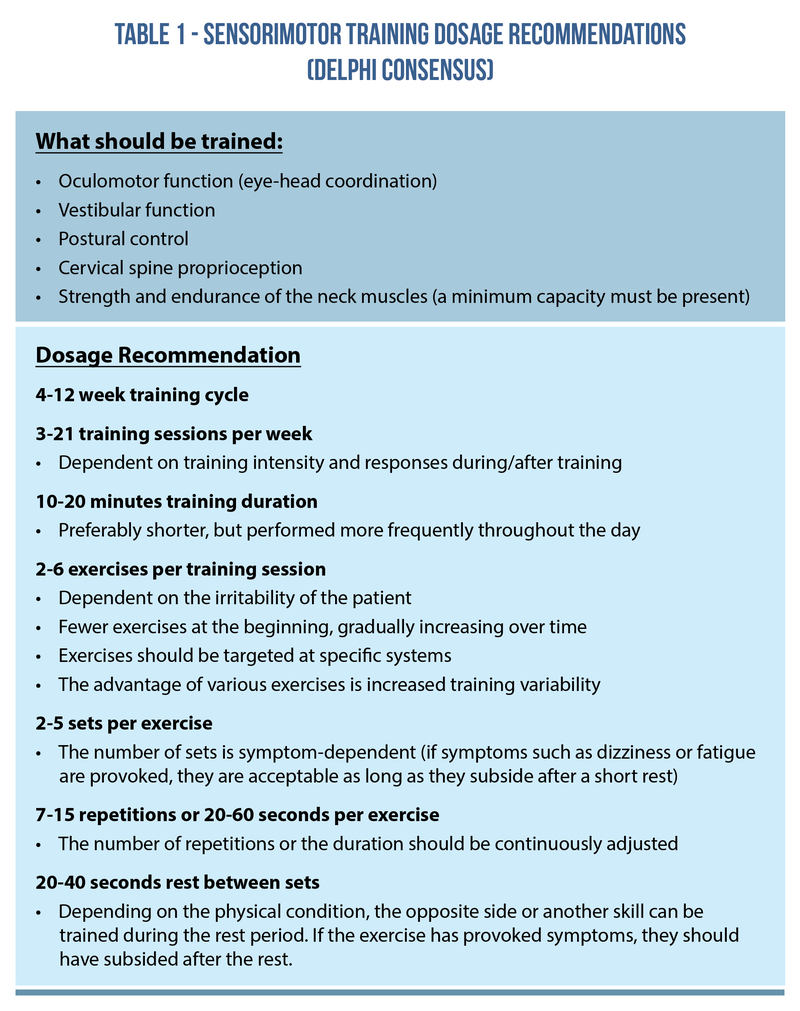
Research Review #3: Sensorimotor Training Dosage for Neck Pain: Delphi Consensus
Finally, this Review provided useful insights into the role of cervical sensorimotor training in people with neck pain and related symptoms.
While Elena didn’t present with dizziness or concussion-related symptoms, the Review reinforced the importance of addressing cervical proprioception and movement control as part of a comprehensive rehabilitation program. I introduced simple joint position sense drills and controlled head-neck movement tasks alongside her strengthening exercises.
The paper also highlighted that exercise dosage should not be rigidly standardised but rather adjusted based on symptom response, fatigue, and patient tolerance. For Elena, this meant keeping these drills brief and purposeful (often once daily), while prioritising consistency over volume.
The broader takeaway from this Review was a reminder that sensorimotor exercises are rarely standalone treatments; they work best when integrated with neck-specific strengthening, education, and manual therapy, all tailored to the individual sitting in front of us.
Treatment plan
Phase 1: Resetting the narrative (weeks 1-3)
Before diving into exercises, the first step was reframing Elena’s understanding of her neck pain. She initially believed her symptoms were caused by “bad posture” or damage accumulating from long workdays. Instead, we discussed how persistent neck pain often reflects load sensitivity rather than structural injury. In other words, her neck wasn’t broken.
In other words, her neck wasn’t broken. It was simply underprepared for the demands placed on it. This shift was important. Because when patients stop viewing movement as dangerous, they tend to move more confidently.
Early rehab focused on:
- Gentle cervical mobility exercises
- Deep cervical flexor activation
- Scapular work
- Frequent movement breaks during work
We also introduced structured work breaks every 45-60 minutes, which helped manage symptom spikes during long meetings.
The goal here wasn’t dramatic change. It was a gradual reintroduction of comfortable movement.
Phase 2: Building capacity (weeks 4-8)
Once Elena became more comfortable moving her neck again, we progressed into strengthening. This phase incorporated findings from research highlighting the benefits of combining neck-specific exercises with upper-quarter strengthening.
Her program now included:
- Progressive deep neck flexor endurance work
- Cervical rotation strengthening
- Scapular strengthening exercises
- Rowing and pulling movements
- Thoracic mobility drills
Importantly, exercises were integrated into her weekly routine rather than treated as a separate “rehab block.” We aimed for three structured strength sessions per week lasting about 25 minutes.
Her headaches began to decrease by week six. By week eight, her daily neck pain dropped to around 1-2/10 on most days.
Phase 3: Returning to full function (weeks 9-12)
By the third phase, Elena was functioning well at work but still noticed fatigue during particularly demanding weeks. Instead of trying to eliminate symptoms entirely, the goal shifted to building resilience.
Her training now included:
- Higher-load upper body strengthening
- Dynamic shoulder and neck control drills
- Rotational movements relevant to tennis
- Cardiovascular exercise to help manage stress
This phase also emphasised stress management and workload awareness. Elena started incorporating short walks between meetings and resumed regular tennis sessions.
Interestingly, she reported that exercise often reduced her neck symptoms rather than aggravating them.
The outcome
By the end of 12 weeks, Elena reported:
- Pain levels reduced from 5-6/10 to around 0-2/10
- eadaches reduced from three per week to occasional
- Improved neck endurance during long meetings
- Greater confidence moving her neck freely
Perhaps most importantly, she stopped constantly monitoring her neck. And that alone made a meaningful difference.
Reflections
Elena’s case reinforced something many clinicians already suspect but research continues to support: Persistent neck pain rarely improves with one magic exercise.
Instead, progress often comes from combining several elements:
- Clear education
- Gradual strength progression
- Movement exposure
- Lifestyle and stress awareness
The Research Reviews helped guide the big picture, but the real progress came from adapting those principles to Elena’s individual situation. Her neck didn’t need protecting. It needed capacity.
Wrapping up
Many patients with chronic neck pain believe they need perfect posture, endless stretching, or complete rest to improve. But more often than not, those strategies quietly slow recovery.
Sometimes the most helpful shift is helping people move a little more confidently and a little more consistently. Because rehabilitation isn’t just about fixing tissues. It’s about rebuilding trust in movement.
If you want clear, practical insights from the latest rehabilitation research, consider subscribing to Physio Network Research Reviews. Each month, expert clinicians break down new studies and explain how they can actually be applied in practice, bridging the gap between research and real-world clinical decision-making.
📚 Stay on the cutting edge of physio research!
📆 Every month our team of experts break down clinically relevant research into five-minute summaries that you can immediately apply in the clinic.
🙏🏻 Try our Research Reviews for free now for 7 days!

Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!