
This blog is a shortened version of a review from the 14th issue of the Physio Network Research Reviews. It highlights a study titled “Criteria for Return to Running after Anterior Cruciate Ligament Reconstruction: A Scoping Review” by Rambaud A et al (2018). It was reviewed by ACL expert Mick Hughes.
Background/Objective:
- There is a lack of high-quality information regarding when ACLR (Anterior Cruciate Ligament Reconstruction) patients can return to running (RTR)
- The primary purpose was to find out what criteria are used in the clinical decision making for RTR following ACLR
- They also aimed to provide information to help clinicians and patients make quality decisions regarding RTR
Methods:
Reviewed 201 studies which included participants ranging from skeletally mature adolescents to those aged 40 years, who had undergone a primary ACLR (autograft only, with or without meniscus surgery)
Results:
- The median time from which RTR was permitted was 12 post-operative weeks
- Apart from “time after surgery”, only 18% of the studies used additional criteria to allow patients to RTR
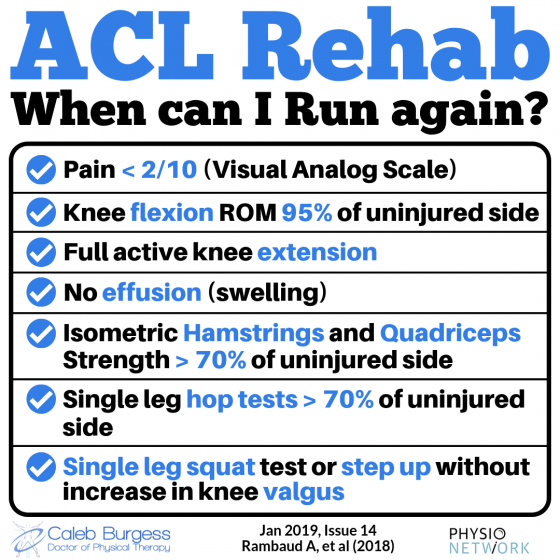
- The most common clinical criteria were full knee AROM and pain <2/10 in the visual analog scale (VAS)
- For strength, the most common objective criteria were isometric quadriceps limb symmetry index (LSI) >80% and isokinetic quadriceps and hamstrings LSI >70%
- For performance-based criteria, the most common objective tests were: proprioception LSI of 100%, composite score on Y-Balance Test >90%, hop test LSI >85%, 10x consecutive single leg squats to 45 degrees knee flexion and 30 step up and holds
Clinical Implications:
- The decision to allow someone to start a running program should be made on passing clinical/strength/functional criteria, rather than being based on an arbitrary time-point
- It should be individualized and for many patients it might be reasonable to commence running between weeks 8-16 post-op provided that there has been adequate progressively loaded rehab
- The patient should have <2/10 pain, full to near full AROM, and little to no effusion
- The clinician may also choose to use a battery of strength and performance-based tests
Want to get better at treating ACL patients?
Dr Hege Grindem has done a Masterclass lecture series for us on:
“Assessing, managing & rehabilitating ACL injuries”
You can try Masterclass for FREE now with our 7-day trial!

Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!