Case Study: Myositis Ossificans – Deadlegs aren’t just for the playground

Whether you call them a “dead leg” or a “Charlie horse” or a “cork thigh” chances are we have all had one. Mostly from the playground days where the bigger kids want to take pleasure in seeing you limp for 5 minutes. However when they happen in sport, with fully grown athletes running at full pace, a collision to the thigh can result in an injury much more serious than the one we associate with from childhood.
The reason I wanted to write this blog was that I worry that thigh contusions are underplayed in the treatment room, potentially because we associate them with those school sports injuries that can be “run off”. This is a case study that I became involved with after initial management of the “dead leg” failed, and to this day is one I reflect on about how important initial management can be in saving severe stress in the long run. This is a case of a “routine” dead leg that is commonly seen in contact sports that resulted in 9-months of rehab to manage a secondary case of myositis ossificans.
What are we dealing with?
There are two types of “dead legs”
- Intramuscular: blunt force trauma to the muscle that results in a haematoma, in this scenario the epimysium remains in tact and the bleeding is contained within the muscle compartment.
- Intermuscular: the epimysium surrounding the muscle is broken along with the damage to the muscle tissue, the resulting haematoma spreads outside of the damaged muscle.
The intermuscular hematoma by far looks the worst, it’s the one where the whole thigh goes black and blue and looks pretty nasty. However, clinically these ones tend to heal quicker and they look a lot worse than they feel. The problem with the intramuscular haematoma is that because it is contained, the pressure can build up and become more painful. It is generally more debilitating as a result, with larger loss of range and more pain. It also doesn’t provide that visible diagnosis as very often you just get a small sign of bruise on the skin from the impact – this is where it can get dangerous as we like to be able to see injuries (hmmm something about invisible injuries and under diagnosis.. concussion?). We have discussed acute management before (here) but with dead legs, it is always worth monitoring for a few days and hoping that the leg goes black and blue.

In the first few days, range is a good indicator. On day 1 after the injury, if they are unable to achieve >90 degrees knee flexion, the prognosis is generally longer. For a bad intramuscular contusion, you could be looking around 6 weeks. This is where the coaches tell you it’s just a dead leg and they’ve had worse. But, it is structural damage to the tissue resulting in bleeding and should be given the same respect you would give to a tear. (Muscle injury classification via the Munich Consensus here).
Myositis Ossificans (MO):
MO is the formation of heterotrophic bone within the muscle following trauma (here) essentially following failed healing the body begins to lay down bone in an attempt to add stability and structure.
Case study:
The following case study is an example of an academy player, where an initial intramuscular trauma to the muscle was accelerated back to activity resulting in a 17cm tear of vastus lateralis (VL), consequently being diagnosed with MO that was estimated to be 3cm thick and of equal length to the tear.
Timeline:
- Day 0 – initial impact to right VL via collision in training, had to be removed.
- Day 1 – “able to squat and lunge but pain on a stretch”. Player expressed determination to train and so was allowed to.
- Day 2-3 – continued training
- Day 5 – Removed from training with “cramp / DOMS” in right leg.
- Day 8 – Sudden loss of power with running and kicking, removed from training.
- Day 30 – returned to training
- Day 31 – played in a competitive game but substituted by manager after 25 minutes due to inability to run. Assessed by doctor and head physio. Visible contained swelling in VL, palpable solid mass, loss of range and pain on contraction of quads. MRI scan demonstrates a 17cm longitudinal tear of VL. Suspicion of MO so sent for ultra sound scan which was confirmed, absent from full team training for 9 months.

Contained haematoma within the vastus lateralis muscle after 30 days of continued training post-initial injury
Management:
Surgical excision of MO is only really reserved for persistent cases that don’t respond to conservative treatment (here). A collective decision was made that we should try to reduce any form of load that may stimulate further bone growth. As a result, the player was removed from all activity of the lower limbs, no soft tissue therapy to the quads and at this stage no stretching of the affected tissues.
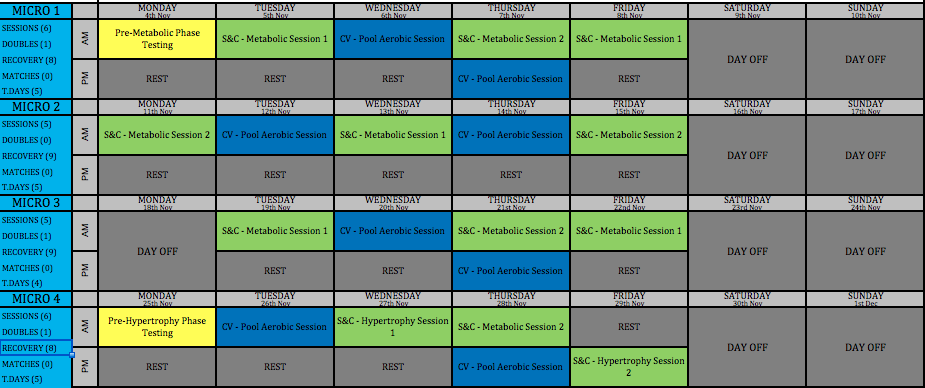
It is neither healthy nor beneficial (or fun!) to completely rest when you are used to training 6 days a week. Credit should go to Will Abbott (@WillAbbott__) for his contribution to the maintenance of the athletic profile for this player. A periodised program was designed to maintain metabolic and cardiovascular systems, strengthen the upper body and completely unload the lower body.
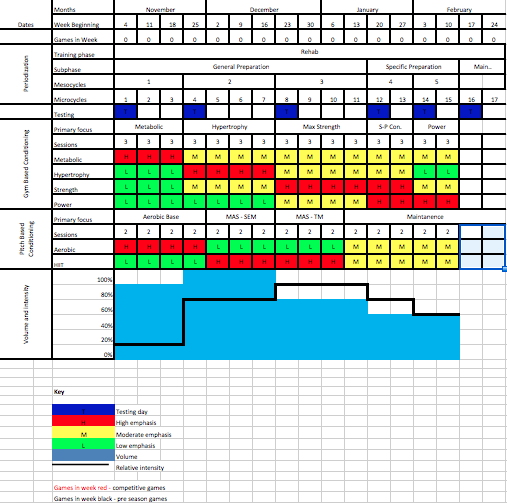
A periodised model to demonstrate maintenance of unaffected systems with complete lower body unload (designed by Will Abbott)
The program included swimming, with multiple floats between the legs to reduce the temptation to kick. All gym based activities were performed seated or with legs supported when lying to reduce axial load through the legs during upper body lifts. Upper body metabolic sessions were implemented via high intensity interval training, with small rest periods to help maintain specific anaerobic demands relating to the sport. This was done using medicine balls, ropes, boxing pads.. anything to reduce the monotony of daily upper body training.
Each month was broken down further (as shown below), with follow-up ultra sound scans every 4 weeks. After the first 4 weeks, we observed a 2.5cm reduction in length which consolidated our thought process to continue de-loading. With limited exercise potential and treatment for the leg, we ran half days and 5 day weeks to help maintain a positive psychological presence.
This was an opportunity to increase muscle mass in the upper body, an opportunity that would not have been possible during season if the player continued to play and train. This allowed a clear progressive pathway for increased lean mass with the following phases:
Hypertrophy –> Max strength –> Strength / power conversion –> Power
While the conditioning phases were as followed:
Aerobic base –> Max aerobic –> Supra max aerobic
There was a decrease in calcicific mass every month, although the rate of this varied each time. By the end of month-4, the mass had completely reabsorbed which meant the reintroduction of load to the lower libs. By this point, the end of the season was 6 weeks away and therefore no realistic opportunity to play again this season, so the decision was made to start physical preparation for the following season.
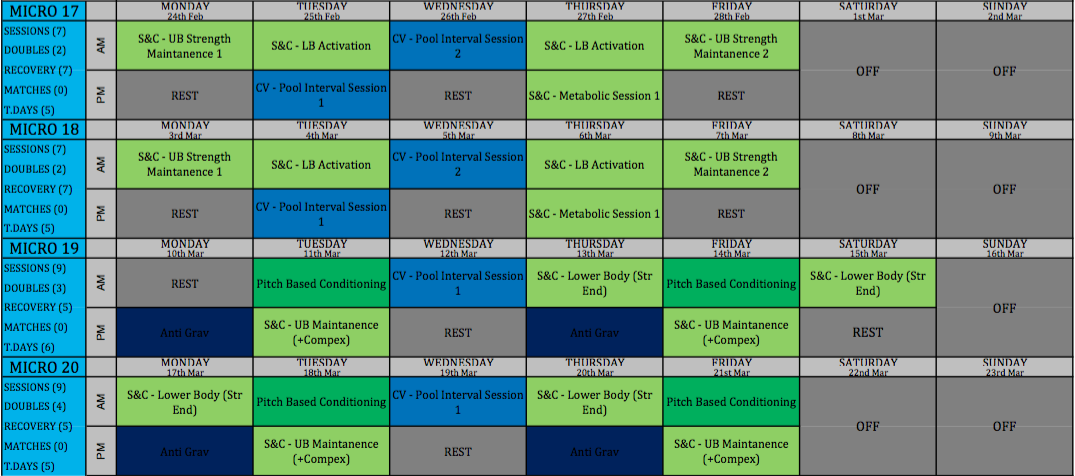
An example of the lower body periodisation
The lower body gym program was tailored as followed:
Strength endurance* –> Strength –> Max strength –> Strength & power complex training
(* This was probably more “re-introduction to the gym” rather than true strength-endurance. But this phase would have served as a gentle hypertrophy phase given the 4 months of atrophy)
Before undergoing a linear outdoor session progressing from general preparation to sport specific drills with Tom Barnden (@barnden_tom). The player completed a full pre-season and no recurrent symptoms to date.
Conclusion:
Hopefully the lengthy timeline of this case study demonstrates the importance of giving each individual injury the respect it deserves. While I hope the management is interesting, the key discussion point is how do we approach “dead legs”? Should there be better education to athletes and coaches about the magnitude of injury? Essentially given the tissue damage, are they a tear? If an A4 piece of paper represented a muscle, and we tear down the middle (strain) or poke a hole through the centre of the page (blunt force trauma), that page is still affected and unable to serve as an A4 piece of paper. Why does the mechanism of damage change the management of injury? Given any loss of range or function following a blunt force trauma, always consider the magnitude of potential damage; monitor swelling, bruising and pain and have adequate timelines in the back of your mind – don’t rush to a diagnosis / prognosis on day 1. There will be times where there is impact and initial pain but full range and full strength – this is where our pitch-side assessment and reasoning comes in (here).
Yours in sport,
Sam
Want to master behaviour change?
Dr Serena Simmons has done a Masterclass lecture series for us!
“Behaviour Change in Clinical Practice: A Physio’s Guide to Psychology”
You can try Masterclass for FREE now with our 7-day trial!

Don’t forget to share this blog!
Leave a comment (1)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Hi, im an osteopath and in no way an expert when it comes to sport injuries or rehabilitation. In this specific case, what are your thoughts on including contralateral lower limb strenght training? Could it have been beneficial? Any contraindications? If yes, at what point, in your opinion, during rehab?