Navigating chronic post-concussion symptoms: Essential strategies unveiled

During my last job, up to 40% of my patients were people with chronic Post-Concussion Syndrome (PCS) or related symptoms. While I acknowledge the term PCS is widely debated, I will use this term for the purpose of explaining some tips for the management of chronic post-concussion related-symptoms throughout this article.
*Side note – even though this is geared towards people with chronic post-concussion symptoms, there is a lot in this article that can be applied to people with persistent pain and acute concussions as well.
Tip #1 – Understand the different demographics
Very few of the actual PCS cases I’ve dealt with are athletes who had an injury while playing sport. Many of these are from workplace accidents or motor vehicle accidents – both scenarios being ones that predict poorer outcomes (1).
Mike Studer has a rocking Masterclass which is geared towards sports-related concussions. It is important though to look at all the different demographics.
I’ve outlined some different factors to be considerate of in the table below:
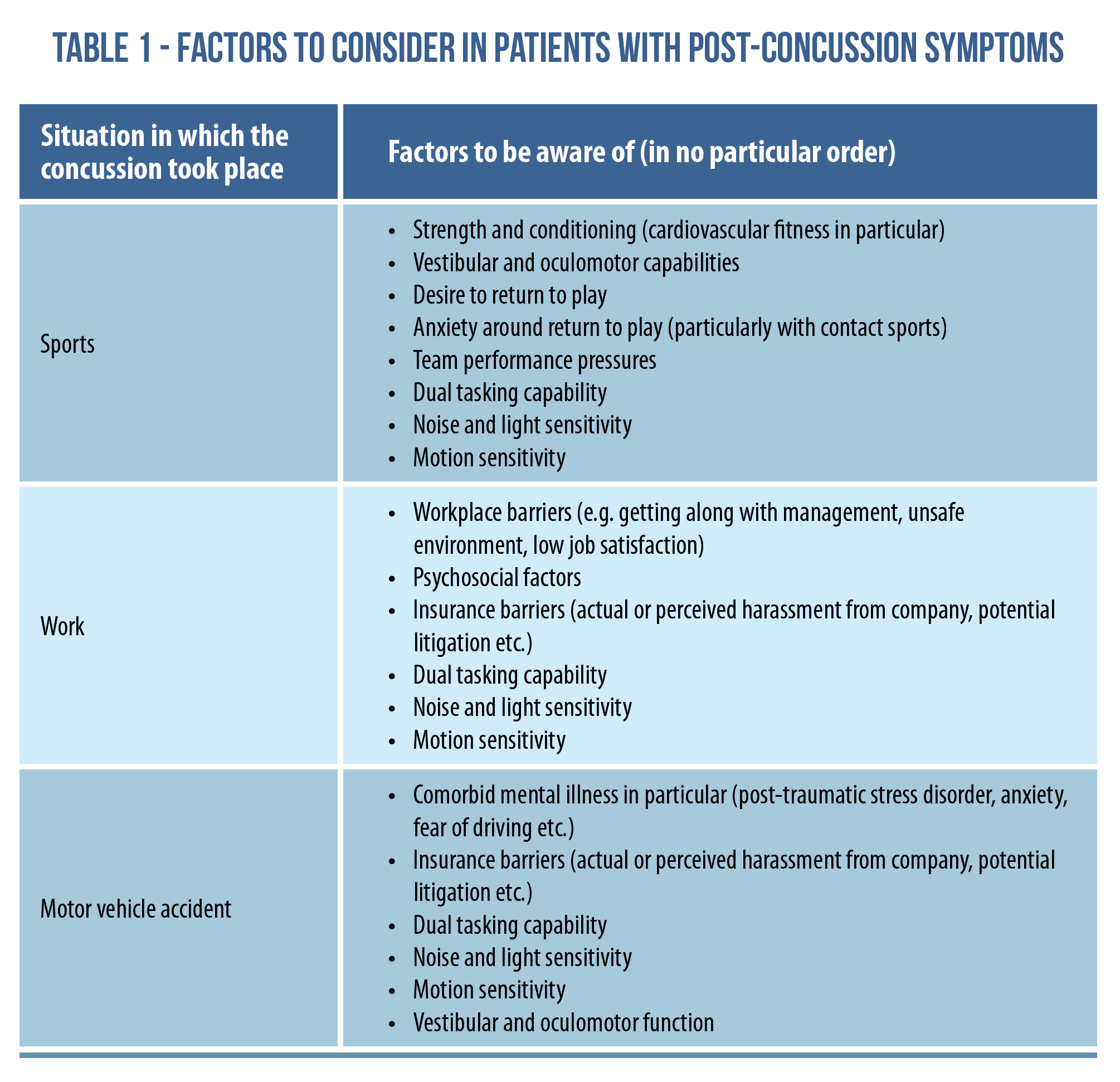
You will see there’s certainly overlap with these different demographics, however there are also different factors which may influence symptoms and success levels. Cognition overlaps with all of these – although it largely falls outside of the scope of practice of physiotherapy, so I won’t spend a tonne of time on it in this article.
*As a disclaimer Mike’s masterclass also mentions that military service, assault and falls are common causes of concussions. I do not want to ignore them, but I must acknowledge that I am not qualified to talk about those demographics in detail.
In one of my favourite Physio Network Masterclasses by Tim Mitchell titled “A framework for optimising the patient interview and clinical outcomes”, he goes through how to clinically reason and determine the presentation of the individual in front of you; including pain presentation, pain mechanisms and contributing factors. While this Masterclass is geared towards musculoskeletal pain, a similar approach is recommended for people with PCS, so it’s worth checking out!
Tip #2 – Get a team involved
In my last job I was blessed to work with neurologists, kinesiologists, occupational therapists, psychotherapists and psychologists, along with other professionals. So many different factors can feed into concussion symptoms and recovery which, depending on the situation, fall out of scope of physiotherapy. These include but are not limited to (another table alert!)…
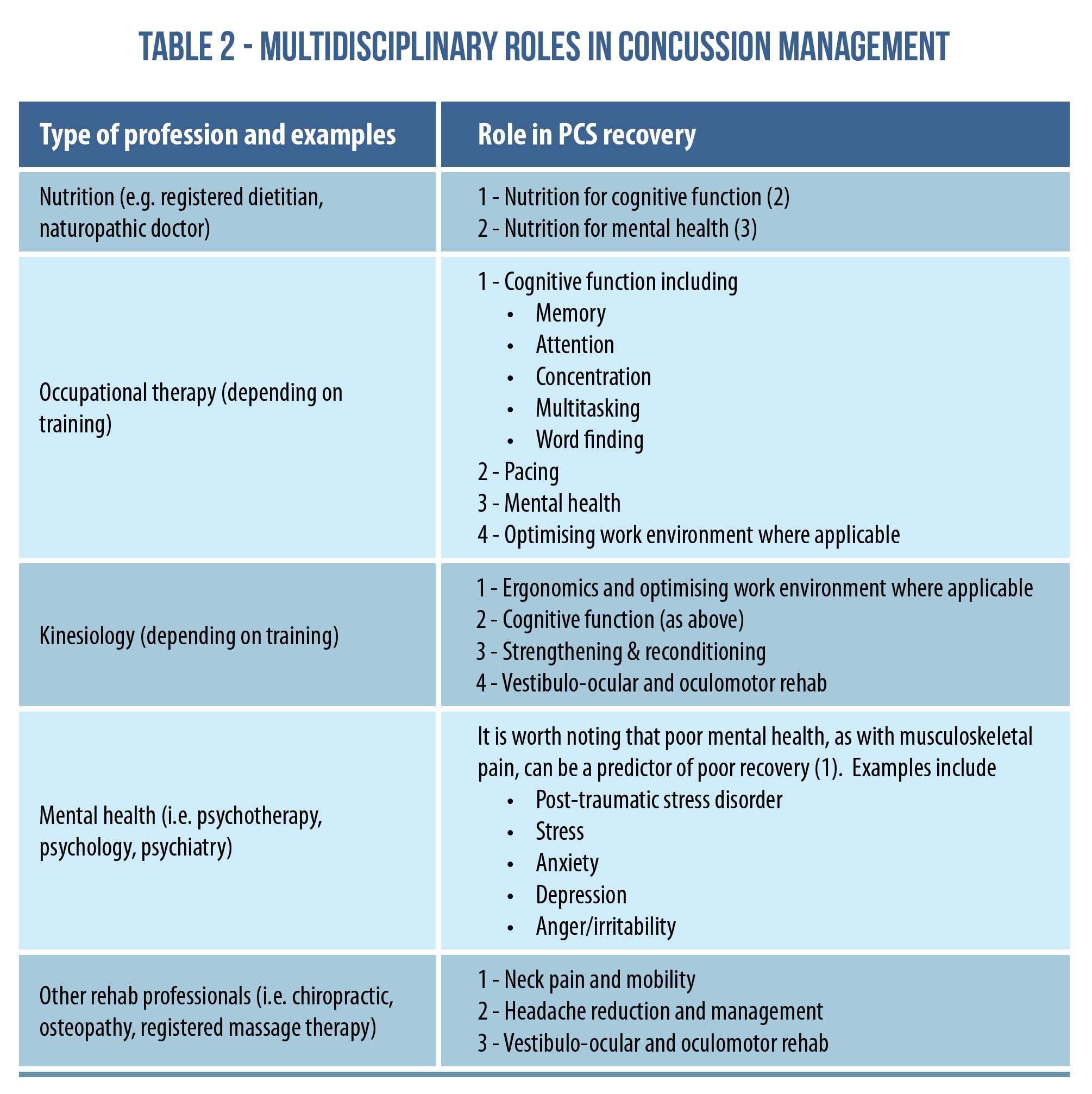
As with the above table, there’s overlap. This illustrates the importance of having a team on your side, whether that be at your workplace, or networking with people outside of your workplace. As I tell people with complex PCS and/or chronic pain who have multiple contributing factors to their symptoms – as a physio, I can only address certain pieces of the pie, and as such, I can’t guarantee full recovery on my own.
Tip #3 – Be prepared to take a lot of time during assessment
In a recent Research Review from June 2023 on slow recovery after sport-related concussion, it was noted that time to recovery, female gender and baseline symptoms/physical function were all factors affecting recovery. With that in mind, it is important to be prepared to take a lot of time to assess, potentially breaking assessments up over multiple sessions. Don’t put too much pressure on yourself or your patients to get everything done in one day!
As Tim Mitchell regularly emphasises in his Masterclass – it’s critical to take the time and listen to the patient to get a proper idea of what is going on and how best to manage it. This gets even more complicated when you deal with clients with a higher intensity of symptoms.

Tip #4 – Have multimodal rather than isolated care
From my experience, a large focus of physiotherapy for people post-concussion is geared toward vestibulo-ocular and oculomotor rehab. This is great and should not be neglected, but there also needs to be focus on goal specific rehab. The patients I’ve worked with who have received unsuccessful treatment for PCS had often fallen short in several areas:
1- Intra-physiotherapy
This refers to the “if you have a hammer everything is a nail approach” of focusing mainly on vestibulo-ocular, oculomotor, and neck rehab while neglecting balance, strength and conditioning, pacing, beliefs about the injury etc.
2- Interdisciplinary
I see this a lot for solo practitioners and unidisciplinary facilities. Sometimes the patients are getting dynamite physiotherapy, however other components such as sleep, nutrition, cognition and mental health are being neglected.
3- Lots of focus on isolated rehab rather than goal focused care
In his Masterclass on concussions, Mike Studer has talked a lot about dual tasking in sporting activities. This is a great and very underrated factor in PCS management. It’s great to focus on balance or vestibulo-ocular rehab, and it’s even better to integrate these with goal activities.
Doubling down on Mike Studer and his other great Masterclass on Behavioural Economics, he also highlights the value of having different approaches to exercise – something that is critical when working with clients who may have had treatment somewhere else.
Tip #5 – Some symptoms are okay
A recent review (4) stated that for acute concussions, past the first couple of days, a small symptom increase of 2/10 (i.e. going from 3/10 at rest to 5/10 with activity) was considered acceptable as long as symptoms came back down to baseline in a timely fashion.
With most, if not all the cases I’ve worked with who have PCS, it’s pretty tough to do anything without a few symptoms. I like to use the above as a guide for treatment.
*Note – some people will be hypervigilant about monitoring symptoms, so this can also backfire. Two alternative approaches are:
- “A small increase in symptoms which reduces relatively quickly is okay”
- Working into a symptom level which is manageable or acceptable for the patient – this is a gem for Mike Studer’s Behavioural Economics Masterclass.
**Each of the above comes with its own strengths and weaknesses, and the choice will be case-by-case, depending on the patient in front of you.
Tip #6 – Task rotation is where it’s at
This is a gem I learned in my last job – rotating different tasks such as cardiovascular exercise, strengthening, vestibulo-ocular/oculomotor exercise or cognitive activities can be very helpful in addressing the important factors while avoiding excessive flare up. It can also (Mike Studer reference alert) be a helpful way of varying and repackaging tasks to get people on board with activities they may not have done before.
Tip #7 – Use caution when administering and interpreting balance testing

I’ve had some PCS patients who, test after test, would not make any improvement with their balance scores. After my own reflection, and discussing this with colleagues, I realised that part of the issue with balance testing came from patients underperforming due to nerves. As an example, I would be standing face to face with another patient and we’d be talking normally, but when I’d whip out the timer and start testing the patient, she’d fall apart. She’s already shown me she can balance in normal and close stance while we’re talking! So I deduced that test-related anxiety can fudge the results. This is a tip that may also be applicable to older adults with balance impairments.
It’s also important to be aware of situations where interpretation of instructions may be an issue. Examples are items six and seven of the Dynamic Gait Index (you can Google it if needed) which require the testee to step over an object without stopping, and to navigate around cones in a specific pattern. Quite often I would see patients perform poorly on these tests, but improve after proper instruction and coaching was given. Again – what looks like a balance impairment may just be a matter of their interpretation!
I don’t like seeing people being written off as having bad balance or being at high fall risk when the issues can be attributed to testing anxiety or poor interpretation of instructions. Don’t get me wrong – I still use balance testing as indicated for people with PCS, osteoporosis, falls/balance concerns, certain lower-limb conditions (e.g. ankle sprains)… however, we need to keep these things in mind in the overall picture.
Tip #8 – An ounce of prevention is worth a tonne of cure
One of the big predictors of chronic PCS is having had multiple concussions (1). In Mike Studer’s concussion Masterclass, I was stunned to see that the risk of having a subsequent concussion is increased by:
- 1.5x after 1 concussion
- 2.8x after 2 concussions
- 3.4x after 3 concussions
So prevention of concussion in the first place is clearly is the best cure!
Tip # 9 – Understand it’s going to take a while
The inherent nature of PCS is that symptoms have carried on longer than normal, and there are likely multiple contributing factors (as outlined above). With that in mind, understand that it can take a few months or more to maximise recovery. This can be compounded more by cognitive and psychosocial factors such as:
- Expectations of a quick fix
- Cognitive rigidity: not being able to adapt and adjust to the current situation
- Concerns of returning to activity
As such, it can sometimes take a month or more just for patients to START to take the steps needed to move them in the right direction.
Wrapping up
Whew, that is a lot! I hope these tips help you in your management of patients with PCS. Remember, as with many chronic conditions, it is a multidisciplinary effort to help the patient reach their goals, and treatment decision-making should ALWAYS include the patient. Thanks for reading!
If you’d like to learn more about how the experts manage concussion, watch Mike Studer’s Masterclass HERE.
Want to become a pro at managing concussions?
Mike Studer has done a Masterclass lecture series for us on:
“Concussion: Assessment and Treatment”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!