Cluster Sets: Leveling up your Exercise Prescription

This blog is going to be a simple, pragmatic clinical guide you can lean on when implementing cluster sets in your clinical rehabilitation practice. Although this is specific to cluster sets, if you want to learn about other methods of rehabilitation, check out the Exercise Prescription in Sports Rehab masterclass by Teddy Willsey.
This blog will aim to cover the following:
- What are cluster sets?
- Where did they originate?
- What are the proposed benefits?
- How can this translate to improving my day to day physiotherapy / rehabilitation practices?
- What patient groups may benefit most from using cluster sets?
To get started, the below diagram highlights a simplistic way to think of a cluster set conceptually:

Taken from (1)
- Decide on a number of reps you were going to do in your normal “straight set” (this depends on the goals of your programming but let’s use 10 reps as the stereotypical physio example). Cautionary note the higher the reps / set the less useful cluster sets get.
- Use the normal load for that rep scheme on that exercise.
- Break your set of (10) reps down into small chunks (or a “cluster”) of reps. Choose a number of reps that would be above a “light effort” on the rpe scale (see image below) with the same load you would normally use for (10) reps.
- In our example 3-4 reps with the 10 rep load.
- Choose a rest interval between clusters (5-45 seconds).
- Perform 3-4 reps, rest 5-45 seconds and repeat 3 times until 10 reps are complete (1,2).
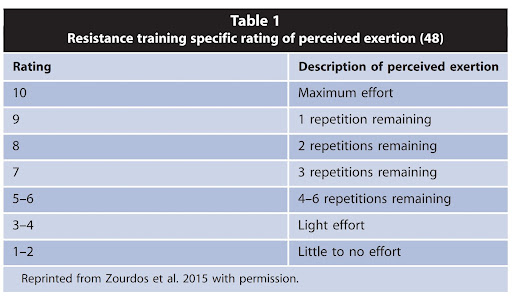
Image taken from (3)
Many physios have used cluster sets for our most deconditioned or painful patients, but without understanding the fundamental principles of why they are so effective. Now you are going to discover the underlying mechanisms and benefits these sets can offer in many different scenarios.
Where did cluster sets originate?
To understand the context from which cluster sets were developed, you have to put on the hat of a 1950’s weight lifter. These people were trying to quickly lift the heaviest possible weight over their head, with good repeatable technique. What they soon found was as reps got higher:
- the more fatigued they were
- the less power they produced
- the more technique degraded
- the less frequently they could practice their skill due to systemic fatigue.
Breaking up each set into small clusters, with short rests, enabled them to maintain technique, be quick and powerful, and minimise the fatigue cost of training.
Since then, cluster sets have seen a great uptake in various team and individual sports that select for speed, power and skill maintenance. This is especially true in periods where fatigue is having to stay low or be dissipated to enhance performance (1,2).
What are the benefits?
Cluster sets have 3 main benefits that we are interested in. To understand these we first have to review the general adaptation syndrome and mammalian stress response.
Definitions:
- A stressor is a stimulus that disrupts an organism from homeostasis (e.g. our rehabilitation exercises).
- Stress response is the magnitude by which the stressor disrupts homeostasis (4,5,6).
Training stressors can be further broken into:
- External stressor. Such as a quantitative measure of physical load (sets x reps x kg’s)
- Perceived stressor. Such as a quantitative measure of how stressful an external event was perceived to be (sets x reps x rating of perceived exertion) (7,8).
It is important to note here that the stress response your rehabilitation stimulus creates is a complex and dynamic interplay between the external stressor, the perceived stressor and the stress tolerance of the organism (7,8).
Anyone who has trained people for a decent period of time intuitively knows this to be true. For example:
- Person 1 does 10 reps of squats with 20kg close to failure.
- Person 2 does the same workout but can lift 200kg.
- For equal RPE efforts, there’s something about all that extra load that just makes it more stressful for person 2.
- Person 2 has a longer recovery time between sets
- Person 2 has less training frequency due to the exponentially greater external stressor and stress response it creates (7,8)

Benefit 1
For an equivalent external training stress, the perceived stressor and magnitude of the stress response is less. This is beneficial as we can apply a useful training stress while incorporating small breaks between sets, reducing the impact of the stressor. One way this works is by making each set slightly less metabolically demanding (9).
Benefit 2
The second benefit is that the power per rep is far greater than that of a straight set. During a “straight set” our rep velocity typically decays as we fatigue from each rep, and usually our initial velocity is slower as the system self-organises to achieve the task of conserving energy to be used across the whole set (1,2,9). In a straight set, each rep utilises a mix of these fibre types to maintain a steady sub maximal velocity. However, we shift to being more type 2 dominant towards failure in an attempt to produce sufficient force (10,11).
On the other hand, with a cluster set the cue is generally given for the performer to lift each rep with maximal intent. This is usually more feasible due to the decrease in cumulative metabolic cost per rep. This means that every rep in a cluster set preferentially trains the bigger, fatigue sensitive type 2 fibres. If you want to know more about this look into the post activation potentiation (PAP), Post Activation Performance Enhancement (PAPE) effects and the size principle of muscle fibre recruitment in relation to rate coding (9-12).
Basically, it takes less energy to create a more efficient neural impulse and muscle contraction for a motor unit, especially bigger type 2 motor units. These fibres have the greatest adaptive potential to help many athletic tasks, as well as reactive balance and agility in older populations.
Benefit 3
The third benefit is motor learning (1-2). Cluster sets allow small periods of rest between sets for the patient to undergo the short feedback loop of motor learning (13). Further technical proficiency seems to degrade under scenarios where fatigue is high, so the small rest breaks help here. This can be ideal for teaching difficult movements or for patients who aren’t so “motor aware”.
Another argument for including cluster sets in your rehabilitation are the trends in recent research regarding neuromuscular adaptations to this type of training. When compared to straight sets for equivalent external stressor volume loads, cluster sets seem to produce equivalent strength and hypertrophy gains. This is despite the fact that these sets aren’t perceived as being as stressful, and appear to disrupt homeostasis less. This gives us more options to reach the same goals in the clinic (9,12).
Practical Applications
So we’ve laid the foundations. Now how do we as rehabilitation professionals use cluster sets to improve our practice?

When I have a patient in front of me, I want to figure out if a lack of capacity to tolerate higher volumes of stress is part of the clinical picture. If so, cluster sets are considered as a potential part of the plan. This can be game changing when trying to help someone struggling to build a bigger cup of tolerance.
Cluster sets can fit really well with the movement snacks and graded exposure approaches to rehabilitation. This is because it allows the patient to explore a movement without the undesired feelings of fatigue.
Cluster sets have been really useful as a bargaining tool where movement experimentation around fear avoidance / painful movements is the goal. Finally, I have found these as a good way to introduce movements, particularly in the paediatric / rehabilitation environment. This is because the set structure allows for greater coaching / learning opportunities.
However, we must consider that performing sets in this way can be very timely. If there are time pressures or you are requiring an adaptation of improved work density then cluster sets will not meet that goal.
I will outline some ways I have used these sets in the clinic for those wanting a pragmatic guide:
- Primary lateral sclerosis.
Main consideration: Fatigue cost of exercise / deconditioning.
Main goal: maintenance of reactive balance and functional mobility.
Exercise prescription: Sit to stands, rack pulls, clock stepping.
4 sets, 3 clusters of 2 reps, 30 seconds between clusters, 2 minutes between sets. - Patellofemoral pain syndrome:
Main consideration: Joint volume tolerance
Main goal: Increasing power / strength.
Exercise prescription: power cleans, trap bar jumps. 2 sets, 3 clusters of 2 reps, 20 seconds between clusters, 2 minutes between sets. - Acute low back pain:
Main consideration: Lack of positional / movement endurance, fear.
Main goal: Promote general movement
Exercise prescription: cobras, hip bridges, cat cows. 2 sets, 3 clusters of 5 reps, 10 seconds between clusters, 1 minute between sets. - Paediatric Rehabilitation:
Main consideration: Low training age, poor motor control, short attention span.
Main goal: Teach rehabilitation while being safe and engaging.
Exercise prescription: Squats, lunges, bodyweight rows. 2 sets, 5 clusters of 2 reps, 20 seconds between clusters, 1 minute between sets.
Wrapping Up
Ok so that’s a wrap. Hopefully by the end of this you feel confident on the practical implementation and clinical reasoning that underlies cluster sets. For more information on rehabilitation in sports, check out the Exercise Prescription in Sports Rehab masterclass by Teddy Willsey.
Want to learn more about sports rehab?
Dr Teddy Willsey has done a Masterclass lecture series for us on:
“Exercise Prescription in Sports Rehab”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!