From Research to Practice: The Gluteal Tendinopathy Rehab Journey

Have you ever wished your patients were as patient as their tendons need to be?
Jessie certainly wasn’t. At 51, she was stronger and fitter than she’d ever been. Two years of consistent running and strength training had given her confidence, energy, and quads that deserved their own Instagram page. But then came the dull ache on the side of her hip- first after hill runs, then during lunges, then just from sleeping on that side.
“I’ve worked too hard to let this sideline me,” she told me during our first session.
And that’s where her story – and our rehab journey – began.”
Subjective assessment: The frustrated runner
Jessie described pain on the outer side of the hip that began insidiously about two months ago. Initially, it was a “post-run tightness,” but by the time she came in, she could barely lie on her left side without discomfort. She’d reduced her running and swapped squats for upper-body days but still felt stuck. No back pain, no pins and needles, no night sweats. Just a deep, nagging ache over the greater trochanter that refused to leave.
Her biggest concern? Losing her progress. “Every time I rest, I feel like I’m sliding backward,” she said. From a psychosocial perspective, that line said it all – Jessie wasn’t just dealing with pain. She was dealing with fear of regression.
Objective assessment: Load intolerance meets compressive pain
On observation, there was a subtle pelvic drop on the single-leg stance. Palpation over the gluteus medius and minimus tendons reproduced her familiar ache. Resisted abduction and FADER (Flexion, Adduction, External Rotation) tests were painful, especially when I added compression. Her hip strength was reduced- about 65% compared to the opposite side on handheld dynamometry. Single-leg bridge and step-down tasks showed slight hip adduction drift and compensatory trunk lean.
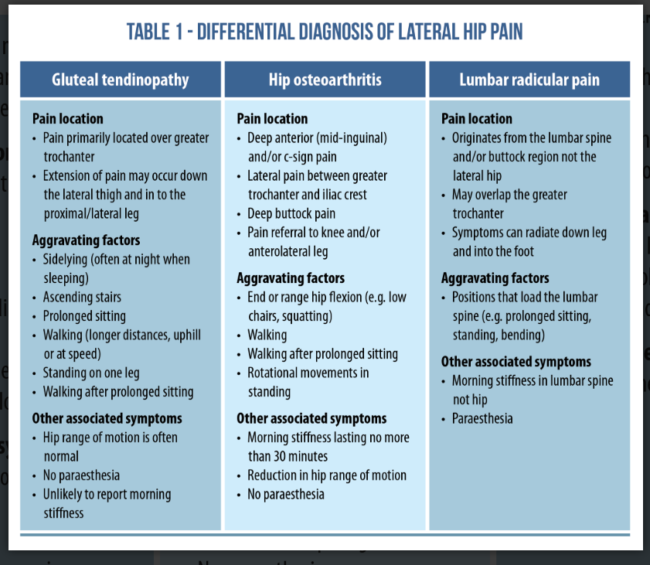
Differentials like lumbar referral and trochanteric bursitis were ruled out. Imaging later confirmed gluteal tendinopathy without a full-thickness tear – a classic case of what many call Greater Trochanteric Pain Syndrome (GTPS).
Navigating the plan: Where research met practice
I used four key Physio Network Research Reviews to guide Jessie’s rehab strategy. Each one offered insights that shaped her recovery timeline and my communication.
1 – Exercise therapy still reigns supreme
This Review reaffirmed something we intuitively know but often forget: exercise-based rehab remains the gold standard for gluteal tendinopathy. It emphasized progressive load management, avoiding compression in early stages, and improving abductor strength and movement control.
So instead of resting, we reframed her plan around “smart loading.” “We’re not avoiding movement, Jessie. We’re choosing the right ones at the right time.”
2 – Hormonal and sex-specific considerations
This Review deepened my appreciation for the midlife female athlete context. Tendon collagen turnover, hormonal transitions, and load capacity can change subtly in women around 50 years.
The message? Rehab should respect physiology, not fight it.
We discussed adjusting her training volume and optimizing recovery, including adequate protein intake and sleep. The research helped me normalize her slower-than-expected healing rate, not as failure, but as biology. Exercise and education were recommended as first-line treatment for hip tendinopathies in this review.
3 – The mind matters; Psychological factors in chronic lateral hip pain
This Review examined psychological barriers: fear of movement, catastrophizing, and frustration, all common in persistent tendinopathies. It mentions that there is a mismatch between how severe the condition is and how the symptoms are presented. Our treatment should not be focused only on the structure at fault but also take into consideration the other health related domains.
Jessie’s anxiety about “losing strength” matched that profile. I integrated graded exposure principles, slowly reintroducing her to movements she feared (like lunges and running). We also used a pain-monitoring model. Pain ≤ 3/10 during exercise and returning to baseline by the next day was acceptable. Framing pain as “information, not danger” helped her stay engaged and empowered.
“You’re not breaking anything, Jessie, you’re training your tendon to trust you again.”
4 – Prognosis and patient expectation in tendon recovery
This Review provided a very important message that pain severity and disability were associated with psychological stress and quality of life. This association was stronger than that of hip abductor strength.
This helped me focus on recovery timelines and patient prognostic communication. Most tendinopathy recoveries take 3-6 months, with some extending to 12. The key predictor of outcome? Consistency, not intensity. This Review highlights the fact that the “just load it” approach might backfire if the rehab process is not taking these psychological factors into consideration and the patient is not being guided towards achieving their goals.
This allowed me to anchor Jessie’s expectations early: “We’re not fixing this in weeks. We’re building durability for years.” It shifted her mindset from chasing a quick fix to embracing a progressive, sustainable process.

Rehab in action: Turning research into real results
Phase 1 – Calm the tendon (weeks 0-4)
Goals: Reduce pain, minimize compressive load, begin controlled isometrics.
- Education on avoiding sustained hip adduction (no crossing legs, side-sleeping with a pillow).
- Isometric abduction holds (30-45 sec x 6-8 reps) to maintain tendon load without aggravation.
- Bridges, clams, and banded abduction at low intensity.
- Cardiovascular alternatives like cycling or upper-body ergometer for conditioning.
She learned that pain-free didn’t mean “no load” – it meant “good load.”
By week 4, night pain had decreased, and she could perform a single-leg stance for 45 seconds without wincing.
Phase 2 – Load it to heal it (weeks 4-12)
Goals: Progress tensile load, improve abductor capacity, and restore functional control.
- Transitioned from isometrics to slow isotonic strengthening (side-lying abduction, single-leg bridge).
- Introduced eccentric-focused hip abduction and step-down drills.
- Integrated glute max strengthening to offload the lateral stabilizers.
- Movement retraining for gait and squat mechanics, reducing hip adduction drift.
By week 8, Jessie was pain-free in daily life and began partial running drills. By week 12, her hip abduction strength was symmetrical within 10%.
Phase 3 – Build robustness (months 3-6)
Goals: Return to running and full strength training without fear or flare-ups.
- Progressive run-walk intervals (starting 1 min run : 2 min walk, building to continuous 20 min runs).
- Plyometric progressions: bounding, small lateral hops, resisted step-ups.
- Reintroduction of gym lifts: loaded squats, deadlifts, lateral lunges.
- Pain-monitoring and weekly “check-ins” to tweak load.
At month 6, Jessie was running her regular mileage and proudly sent me a photo mid-stride, captioned: “Zero pain. 100% sass.”
Wrapping up
Jessie’s case reminded me of something simple yet profound: we don’t just treat tendons, we coach nervous systems, beliefs, and lifestyles.
Research gave me the structure, with load progression, pain thresholds, timelines. Jessie gave me the lesson: progress is rarely linear, and empathy accelerates healing as much as exercise does.
When she finished, she said, “I didn’t just get my hip back. I got my confidence back.”
And that, to me, is the definition of evidence meeting humanity.
Want to keep blending evidence with empathy in your own practice? Physio Network’s Research Reviews turn the latest findings into real-world results – because great rehab starts with great information.
📚 Stay on the cutting edge of physio research!
📆 Every month our team of experts break down clinically relevant research into five-minute summaries that you can immediately apply in the clinic.
🙏🏻 Try our Research Reviews for free now for 7 days!

Don’t forget to share this blog!
Leave a comment (2)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
the post “Patellofemoral Pain: Running Gait Retraining Explained” on the Physio Network site breaks down how a thoughtful gait retraining program can turn around persistent knee pain in runners.
Physio Network
I appreciate that the author emphasizes education, movement pattern adjustments, and gradual progression rather than only strength work.
Physio Network
The case study of a 31-year-old runner who improved dramatically under this approach adds real-world weight to the theory.
Physio Network
https://yacinetvpro.com/
After such insightful reading, I’ll probably relax with Yacine TV for a bit of downtime — thanks for sharing!
Small remark: Good structured review, however. Anxiety for “losing strength” does not relate to the Fear – Avoidance Model in Pain Science. Moreover, this approach is not progressive exposure, but progressive comprehensive capacity increase based on different demands – which is a great way to – “Calm things down and build them up again”.
Where very often psychological co-factors are involved (we treat people), they have much less often much to do with the specifics of the rehab strategy. Such pain specific approaches would not be more beneficial as a simple Education, Support and Capacity Increase – in the normal borders of tissue healing and inflammation.