Leg pain unveiled: It’s not always sciatica!

Leg pain is a frequent complaint in physio clinics. All too often it’s brushed off as “sciatica”, but the poor sciatic nerve isn’t always the culprit. Leg pain can have somatic, neuropathic, vascular and systemic causes, which makes assessment complex to say the least! Identifying the correct cause of pain is important, as every diagnosis requires a different treatment approach. This blog will cover some of the main differential diagnoses of leg pain and how to recognize them, so next time someone comes to your clinic complaining of leg pain, you’ll know better than to simply label it sciatica.
If you’re interested in this topic and want to dive in deeper, I recommend you watch expert physio Charlie Clements’ Masterclass on spine-related leg pain HERE.
Somatic drivers
Low back
As many as 60% of people with leg pain also complain of low back issues. But knowing which structure might be responsible for the leg pain isn’t so simple. Nerve roots, discs, facet joints, the SI joint… They can all cause pain in the legs! Treatment depends on whether the pain is somatic or neuropathic, which is why one of the first questions to answer is whether the leg pain is referred or radicular. Luckily, each comes with their own specific pain experience. Referred pain is typically diffuse, dull and achy. It usually follows a mechanical pattern and pain is often much worse in the back than it is in the leg. On the other hand, radicular pain is much more localized and, contrary to popular belief, doesn’t always follow dermatomes (only one third of cases do!). Patients complain of shooting, burning pains which are capricious, and aren’t necessarily provoked by specific activities or movements. The leg pain is usually more bothersome than the back, and neurodynamic testing will most likely be positive.

Hip osteoarthritis (OA)
Pain caused by hip OA is often felt in the greater trochanteric, groin or buttock region, but can refer more distally (even below the knee). The fact that hip and low back pain have overlapping symptoms makes for a tricky differential diagnosis. Additionally, hip and low back pain are often concomitant, which makes it even more complex. However, if your patient is limping, they are 7x more likely to experience hip than back problems. Groin pain is 7x more likely to come from the hip than the back, and if there’s an additional internal rotation deficit, chances are even higher that the hip is the main culprit! Some of the more functional features include pain that is worse in the first 30 minutes of the day, catching/clicking sensations, instability, and pain with putting on socks/shoes and getting in/out of the car.
Greater Trochanteric Pain Syndrome (GTPS)
This will often cause referred pain in the lateral leg. It affects females more than males and there appears to be a correlation with chronic low back pain, as up to 45% of people with GTPS also complain of low back symptoms. GTPS often arises after a change in load/activity and elicits pain with side lying, cross-legged sitting and ascending/descending stairs. Recent findings suggest there might be a connection between GTPS and decreased estrogen levels, which could explain why females during and after menopause are more prone to suffer from the condition.
Deep Gluteal Syndrome (DGS)
You might know this one better as Piriformis Syndrome. DGS is a non-discogenic entrapment of the sciatic nerve within the subgluteal space, which is basically an umbrella term whereby a multitude of different structures can create many vague symptoms in this area. PGS will typically cause buttock and retro-trochanteric pain which is provoked by sitting, palpation of the buttock, and passive and resisted hip movements.
Neuropathic causes
Sciatica
Sciatica is the first thing a lot of people think about when experiencing leg pain. It isn’t as common as we think though, with only 2-3% of the population in the UK being diagnosed each year. However, it’s important to guide people with sciatica appropriately, as they typically experience worse pain, and have higher risk of poor outcomes. What makes sciatica so difficult is its heterogeneity – you may have already noticed from experience that no person with sciatica has the exact same symptoms. What’s most important is recognizing the general symptoms of radicular pain we’ve already described above: leg pain worse than back pain, usually distal to the knee, with objective neurological findings and neuropathic pain qualities. Unfortunately, the dermatomes we’ve so carefully studied in school aren’t always very accurate when it comes to this condition – things like thermal or mechanical hyperalgesia and sensory loss may affect some but definitely not all people with sciatica. Pain is most typically felt in the calf, then foot and lastly knee/thigh region. One of the key messages to give people with sciatica is that it needs time; 90% of people are thought to improve within 4 months, but one third of people continue to have symptoms after a year.

Lumbar spinal stenosis
This is present in up to 60% of adults over 65 years old. The majority are asymptomatic, but the ~11% with symptoms experience significant pain and disability. If your elderly patient tells you their symptoms are aggravated by standing and walking, and reduced by sitting and bending, then chances are high that they’re caused by spinal stenosis. Other symptoms include cramps and aches in the legs, balance issues and paresthesia.
Vascular culprits
Peripheral Artery Disease (PADS)
This affects a large percentage of the population. A partial or total blockage of the blood vessels reduces blood flow to (mostly) the lower limb, causing exertional leg pain which occurs only during movement. People with PADS are often plagued by other comorbidities like coronary heart disease, diabetes or stroke, but there’s also a strong genetic predisposition. Symptoms are often bilateral, and the patient’s skin usually looks different than normal (think: hairless, smooth, possibly dry, mottled, reddish).
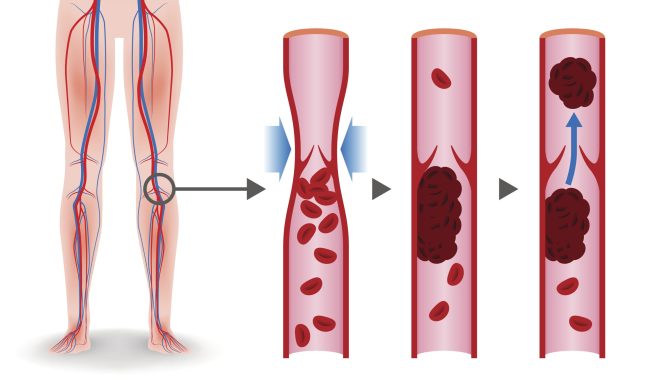
Deep Vein Thrombosis (DVT)
This is something that should be referred on for medical investigation. A DVT occurs when a blood clot forms in one of the deep veins, usually in the lower limb. It can affect everyone, but is more likely in pregnant women, people with comorbidities like cardiovascular disease, or after long periods of immobilisaiton (e.g. long-haul flights). If your patient complains of warm, heavy, swollen legs (>3cm difference between sides) alarm bells should start to ring, especially if the person has undergone surgery in the last three months, or been on a plane in the past three days. If the clot loosens and starts to travel through the bloodstream, it can cause major problems such as pulmonary embolism or stroke.
Systemic drivers
Peripheral neuropathy
One of the most common causes of peripheral neuropathy is diabetes. Symptoms are mainly sensory, but can also include autonomic features and weakness. Diabetes has a predilection towards the smaller C and A delta fibers, which are responsible for temperature and sharp/blunt sensation respectively. However, 75% of cases will also involve the larger A alfa and beta fibers which play a proprioceptive role. People with distal peripheral neuropathy will complain of pain, tight and achy feet or legs, and they may feel as though they are walking on sponges. Ataxia and weakness can be present in more severe cases. Another important cause of peripheral neuropathy is vitamin B12 deficiency. Vitamin B12 comes mostly from dairy, meat and fish which is why it is a common deficiency in vegans, but is also regularly seen in the elderly with gastrointestinal disorders and as a result of certain medications (e.g. proton pump inhibitors).
Exertional rhabdomyolysis
Exertional rhabdomyolysis is a rapid breakdown in skeletal muscle after (intense) physical activity. Its typical features include weakness, acute muscle pains of high intensity, and a dark, tea-like urine colour. More systemic features such as fatigue and malaise can also be present.
Wrapping up
As you can see, there’s a multitude of conditions (other than sciatica!) which can cause pain in the legs. It’s important to have a good understanding of what the source of leg pain is, so you can develop an appropriate management plan.
If you would like to learn more about spine-related leg pain causes and treatment strategies, watch expert physio Charlie Clements’ full Masterclass HERE.
Want to get better at differentially diagnosing leg pain?
Charlie Clements has done a Masterclass lecture series for us!
“Spine-related leg pain: from root causes to treatment strategies”
You can try Masterclass for FREE now with our 7-day trial!

Don’t forget to share this blog!
Leave a comment (1)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Thank you for this insightful blog on myotherapy! I’ve always been curious about how this form of therapy can effectively address muscle pain and tension. Your detailed explanations and practical tips have shed light on the benefits of myotherapy.