
When you think of people hurting themselves while lifting weights, back pain is usually the first thing that comes to mind.
In this article I discuss the long and winding topic of back pain in the lifting audience. This article will be more biomechanical in nature and is very influenced by Stu McGill’s research and work – which I highly recommend you read (at least read his main books Low Back Disorders along with Ultimate Back Fitness and Performance). I do find,, that the weight training clients I work with who have back pain tend to have more nociceptive drivers to their pain in comparison TO other clients dealing with back pain.
What about psychosocial factors and pain?
Anyone who follows my work knows that I’m a big believer in comprehensive biopsychosocial rehab. Before I get tarred for not discussing psychosocial factors in this article – I bring up psychosocial factors in my foundation piece here which I recommend reading before getting into this. It is important to understand that:
- Comorbid mental illness (i.e. anxiety, depression, ptsd) and maladaptive beliefs about the back (i.e. movement and activity being harmful, the back being severely damaged and in need of rest or injections or surgery) can be MAJOR risk factors for chronic back pain (1).
- It’s also critical to take into account what kind of information your client has gotten from other providers, fellow lifters, and the Internet. It’s not uncommon to see lifters bounce from person to person and sometimes develop nocebic beliefs (2).
- There can be a lot of apprehension with returning to lifting after injury and with adding weight to the bar.
- Also coaching should be done, as often as possible, in a positive fashion to help get what you want out of your clients without inducing fear (3).
With respect to psychosocial factors and pain, I highly recommend looking at the Masterclass, A framework for optimizing the clinical interview and patient outcomes by Dr. Tim Mitchell.
Loading factors and back pain
Before I am criticized for citing a paper that doesn’t link mechanical factors and back pain, here are some issues with that argument.
- Some research does link mechanical loading factors and low back pain (4)
- Some of the articles look more at occupational loading and don’t have the same level of load involved as a lot of the clients I deal with. Research may prove me wrong in a few years, and I’m OK with that, but I have an extremely hard time extrapolating research done on boxes weighing <100 lbs to a 600-700 lb barbell.
The three main mechanical loading factors that I’ve found can aggravate back pain are
- Compression
- Flexion
- Extension
Some would argue shear as well but that is a discussion for another time…
Compression
Compression applies usually to two things:
- Quite simply the load on the bar – I see this sometimes during barbell lifts where clients, despite having textbook “perfect” form, may still report back pain particularly after weight has been lifted at or above a certain amount.
- Higher level of muscle co-contraction – particularly through the abdominals and spinal musculature: this can be through:
- Straining to complete a lift or what some therapists call a “high threshold strategy”.
- Exercises that require more co-contraction through the back and core: Examples of these include anti-rotation movements such as Pallof Presses and Anti-Lateral flexion movements such as Suitcase Carries.
- Excessive muscle tensing or guarding as a protective act: This is a big example where psychosocial factors and beliefs can influence physical loading.

As an aside – bracing is a controversial topic in the back pain world. It all depends on whether bracing makes back pain better or worse – that will have to be tested in each individual.
Strategies to deal with compression are
- Proper progression of loading the bar and deloads. Progressing load on the bar by 5-10% at a time is a good progression although some can progress faster and some need to progress slower. I generally am a fan of deloads every 3-5 weeks as a preventative measure.
You can also progress in ways other than adding weight such as:
- Density: doing more work in a given time period or doing the same work in less time (as long as form isn’t compromised)
- Adding in more volume by adding more sets
- Adding more volume via higher reps. Some respond better with sets of 4-8 or 5-10 than the classic 1-5 rep range used in barbell strength training and powerlifting. The only catch with this is to keep the form good as sometimes this deteriorates with higher reps.
- Adding slow eccentrics and/or pauses to the movements.
- Pick a weight you can handle with good form and not push past technical failure.
- With regards to core exercises I like strength coach Mike Robertson’s saying of “master the sagittal plane first” (5). This means mastering sagittal plane core exercises (i.e. Planks, Birddogs, Mcgill Curl-ups) before progressing to frontal plane (i.e. Suitcase Carries, Side Planks) and transverse plane exercises (i.e. Pallof Press, Cable Chops/Lifts). This helps both from a technical perspective as the latter movements tend to be more complex and also from the perspective of getting people used to spinal loading.
- Proper coaching on when and how to brace: It’s one thing to brace during heavy barbell lifts but you shouldn’t be bracing during a dumbbell Bicep Curl or Front Raise. This can be due to too much weight and pushing past technical failure but can also be a result of fear of exercise and fear of lifting weights. This is where things like pain science education, reassurance and graded exposure approaches can come in extremely useful.
Flexion
No, I don’t think flexion is the big, bad boogie man that it’s been made out to be. But the vast majority of lifting clients whom I work with who have back pain are predominantly aggravated by flexion. Exercises such as Sit Ups and Crunches tend to exacerbate more than help symptoms and lifting technique that involves a large amount of visible flexion (you can never 100% eliminate it) can be very symptomatic for these athletes.
I think that load management and being cognizant of cumulative flexion volume is appropriate. However, if I can get people lifting without pain by simply reducing flexion during a lift then this is an obvious win. I’ve lost track of how many clients who have flexion-aggravated back pain and feel better by tweaking their lifting technique, eliminating the lumbar flexion stretches (at least temporarily) and by replacing dynamic ab exercises (i.e. Sit Ups) with more static exercises (i.e. Planks).

Extension
Extension can be a trigger for some with certain exercises such as the Hyperextension exercises (Superman, 45-degree Back Raise, Reverse Hyper). More often than not, they’re done improperly due to a lack of mobility in other areas (i.e. hips, shoulders, thoracic spine), too much weight, pushing past technical failure or just poor body awareness. Common exercises on this list include Squats, Deadlifts, Curls, Shoulder Presses, Lunges/Split Squats, Rows, Shoulder Raises, and Bench Press).
The simple ways to work around both flexion and extension include:
- Modifying the exercises to minimize extension and flexion (i.e. using a shorter range of motion on a Reverse Hyper)
- Using the cues I have outlined in my “Best Damn” Squat and Deadlift articles
- Doing mobility work on potentially limited areas such as hips, ankles, shoulders and thoracic spine.
- Reducing the amount of extension exercise to one that’s tolerable and building up slowly. An example of where I have to do this is with gymnasts – they have to flex and extend the spine to do gymnastics so I have to work with that and appropriately load manage to help them get to where they want to go.

Problematic exercises and modifications
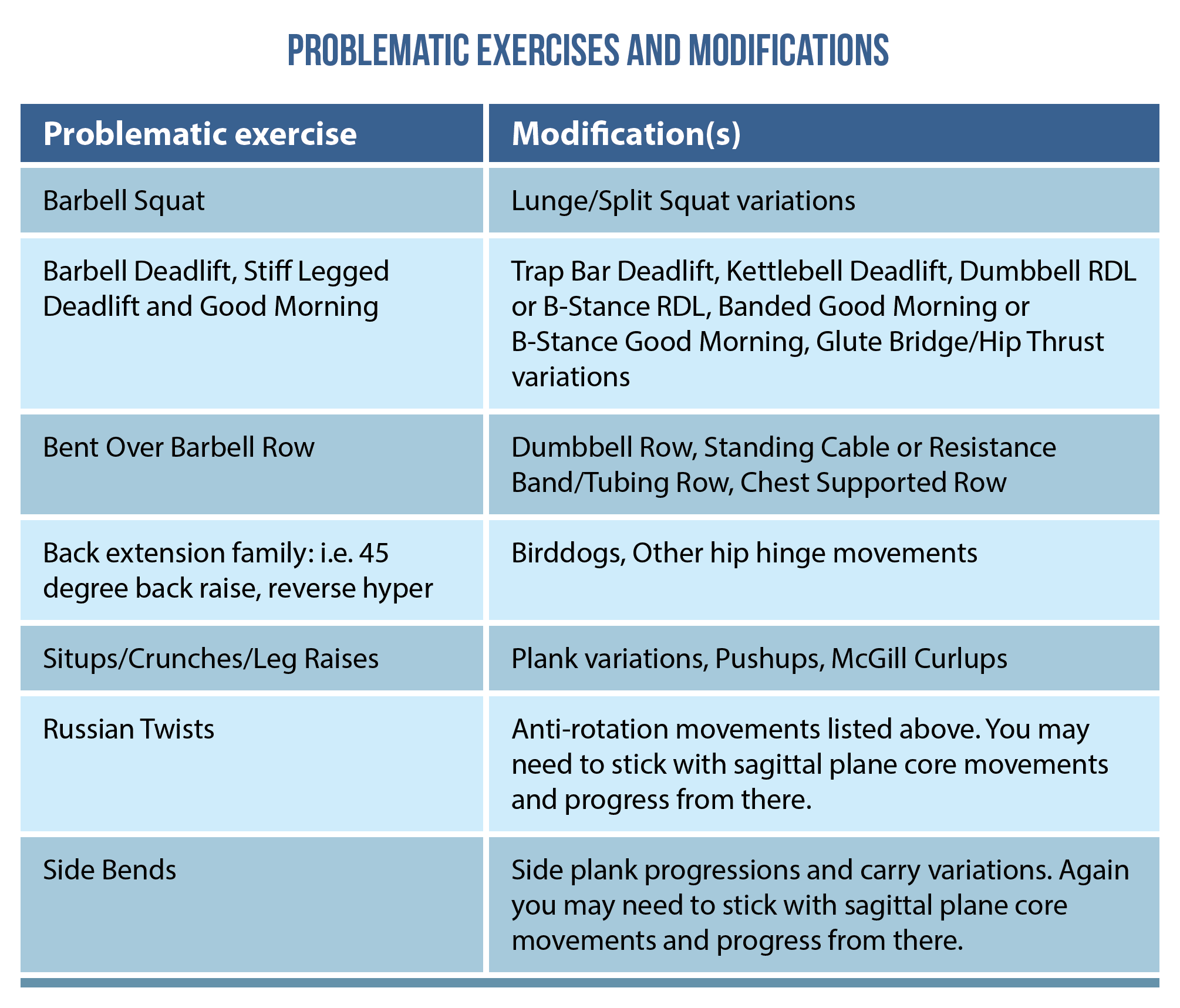
What about activities where I have to bend the back?
Now some activities, such as strongman, crossfit, and gymnastics, require flexion and/or extension of the back – that is unavoidable.
In those situations, particularly with high level athletes, my recommendations in a very Stu McGill influenced style are to:
- Minimize the amount of spine flexion/extension through the day in order to “leave more in the tank” for those demanding tasks.
- As with other movements and other joints, effectively manage the workload of those activities.
Wrapping up
Whew – so if you’ve gotten through this long winded piece, then congratulations!! Stay tuned for the rest of this series where we discuss lower limb pains in the lifting audience.
Before my next blog, check out this masterclass, A framework for optimizing the clinical interview and patient outcomes by Dr. Tim Mitchell.
As always, thanks for reading!
Want to learn how to master the subjective examination?
Dr Tim Mitchell has done a Masterclass lecture series for us on:
“A framework for optimising the patient interview & clinical outcomes”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Leave a comment (1)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Bakker et al. (2007) conclusion is:
“Mechanical loading of the spine, quantified with the 24HS, at baseline is not a prognostic factor for chronicity or recurrent episodes. Possibly modification of spinal mechanical loading in terms of 24HS scores might be beneficial for secondary prevention in patients with acute LBP.”
I am not sure we can extrapolate and write “Some research does link mechanical loading factors and low back pain”