
If you know anything about my philosophy you’ll know I’m a big fan of Mechanical Diagnosis and Therapy (MDT), aka the McKenzie method. It is a very popular method of physical therapy and is #2 behind the Maitland method in terms of the number of research studies done on it (1).
During one of my clinical placements I worked with several strict McKenzie therapists – including Richard Rosedale who teaches many of the courses and have also done some (not all thanks to covid, course cancellations and other matters) of the courses & continue to read the literature and case studies on the method. I’ve (anecdotally) had a lot of success with MDT with many patients, but have also learned some useful lessons (some of which I’ve written about in one of my most popular articles (2)), and made some modifications to it along the way that I’d like to share with you in this blog. As a disclaimer, this is predominantly anecdotal in nature and is an extension of an article I wrote a few years back (3).
As a side note, this article assumes that you have a basic knowledge of MDT. If not – I’d recommend at least taking their free online preliminary courses and reading whatever books, research and case studies you can to at least get a basic idea of how the method works. Unfortunately many therapists only understand the “bastardized” version of MDT and not the whole method. It is an assessment and clinical reasoning method, not a generic set of exercises.

The main ways I’ve modified the McKenzie method for better outcomes with my patients are:
1 – Being selective in whom I use repeated movement testing with
If you read the McKenzie books you’ll know that MDT is contraindicated in inflammatory pain conditions (i.e. acute pain less than a week or two old; or constant pain that’s aggravated by everything).
I’m also hesitant to use it with clients who have constant, diffuse pain; heavy psychosocial factors; and pain with pretty much everything during my base exam. MDT has a “chronic” classification for clients that fit into this category. If I’m 99% sure they’re gonna end up here, then why risk potentially flaring the patient up and them not returning?
That said – MDT can still be used with people with persistent pain. I just start more gently with them and often (particularly for spinal pain) start with static positioning first and then (if positioning doesn’t work and doesn’t exacerbate symptoms) do very low rep repeated movement testing (sets of 5 to start). This helps me assess if further MDT testing is worthwhile or if it’s just not going to give the desired effect.
2 – Being selective in how much repeated movement testing I use in one session
Two of the disadvantages of the McKenzie method are:
- It can be easy to flare clients up with a lot of testing.
- If you don’t find a directional preference it can make you look incompetent and cause the client to have less faith in you and/or themselves.
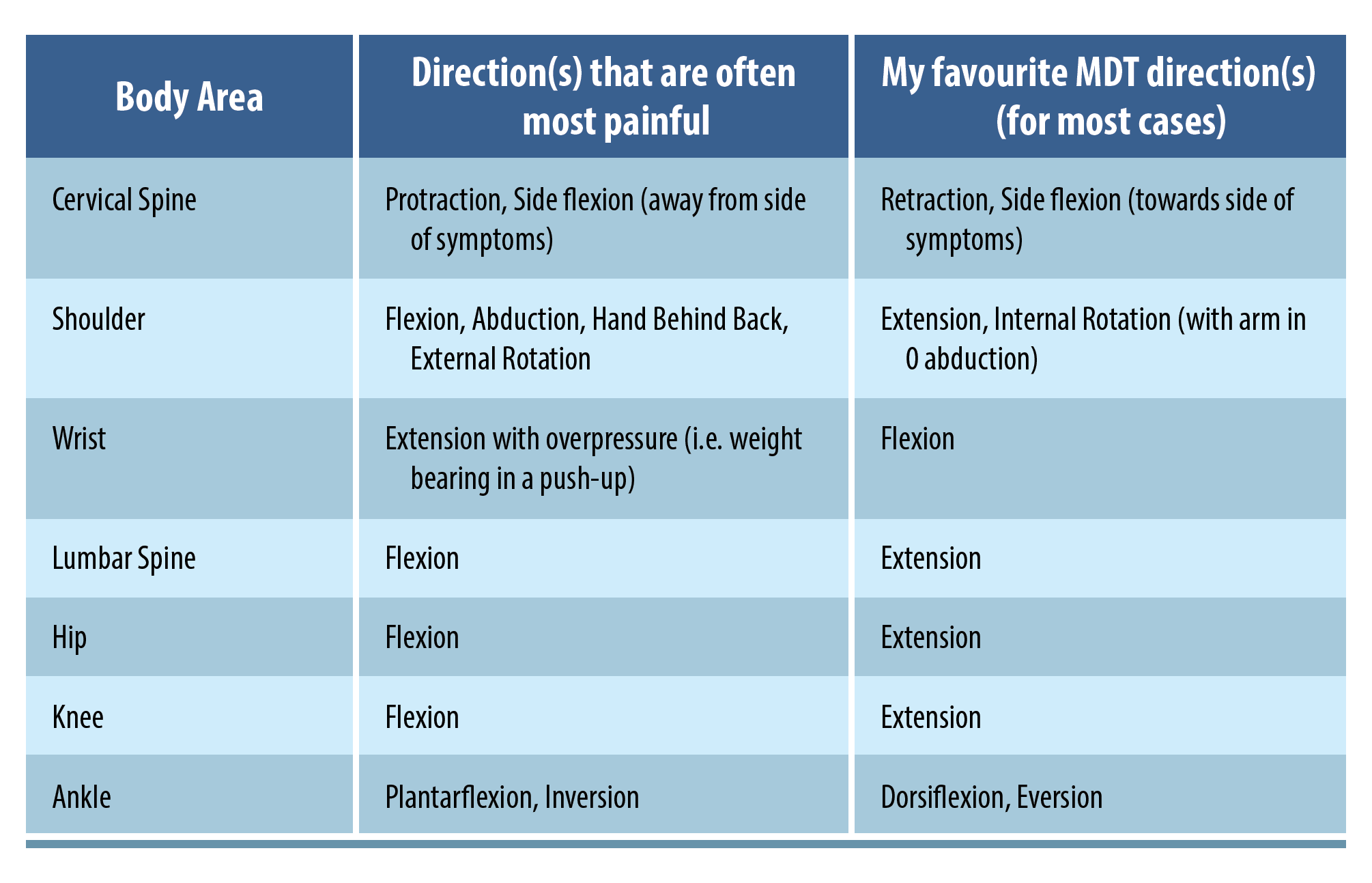
If it’s a client with whom I’m concerned about flaring up during an assessment, I’ll often just test 1-3 directions (at the most). If they don’t respond well to any of them I’ll call it a day and look to test more on the next session. Below are my favourite (and least favourite) directions for repeated movement testing…
Also, if a client doesn’t have a directional preference it is critical to reassure clients that they can still do quite well even without a directional preference.
3 – Modifying types, volumes, and frequencies as needed to help with adherence
When it comes to exercise for pain, the name of the game (other than tolerance) is adherence. The best exercises in the world are no good if your clients can’t stick to them. With that in mind – I tend to shy away from exercises that require lying down unless your patients are in a work situation where they can lie down to knock out their repeated movements multiple times throughout the day. Almost all of the repeated movement exercises I give can be done in sitting and/or standing.
Volume per set is also important as some clients, particularly ones who are very deconditioned, may get tired doing sets of 10 throughout the day. In those situations I may have them do sets of 5 or even give them a “repetition quota” for the day (i.e. 30-40 reps per day) that they can spread out however they see fit.
Lastly, frequency is also a major consideration. While repeated movement exercises are often to be done for 10 reps every 2 hours; I like to start more gently (i.e. 10 reps, 3-4 times/day spread out), assess progress, and adjust up or down from there.
As an aside: if you’re interested in learning more about how to prescribe exercise for people with pain, check out Ben Cormack’s Masterclass.
4 – Using it as part of a comprehensive model
A big myth about MDT, often shared by people who are less knowledgeable about the method, is that it ignores psychosocial factors. In reality, the method looks a lot at psychosocial factors (particularly in its books), which is quite amazing considering that a lot of the material came out well before the biopsychosocial model started to make it into mainstream therapy this past decade.
That said – there are other factors to look at including:
- Workload management/activity modification: Your client may respond well to knee extensions with overpressure but if they’re running 20 km per week and can only tolerate 10 km per week you may be limiting your progress. Also if they stop running, do the repeated knee extensions, abolish their symptoms, and jump back up to 20 km per week you may go in circles. An appropriate progression of activity volume is needed.

- Neuromuscular control: This is just a fancy term for how you move. I’ve lost track of how many clients I’ve had with back pain who don’t tolerate flexion, respond well in the clinic to extension, and the next day come back unchanged or even worse. When I ask them about their activities and get them to demonstrate how they do those activities they move in the exact way that worsens the symptoms. Proper coaching and cueing of the desired movement, and (if needed) aids such as taping may be useful to help the client move in ways that allow for symptom reduction.
- Kinetic chain function: While concepts like the Joint By Joint and Regional Interdependence model are far overdone, sometimes a lack of mobility/strength/control at one joint may influence pain at another joint. The most easy example to think of in this regard is your client who has back and leg pain with flexion that has stiff hips and ankles and has to bend through the back every time he/she bends over. While repeated extensions may make their leg pain centralize, if the hip and ankle mobility deficits aren’t addressed the client may not be able to fully allow her back to desensitize, and may keep re-aggravating the issue and going in circles.
- Overall strength & conditioning: A sprained ankle may do well with repeated eversions, but without proper strength/stability the client may not have the ability they need to run and jump on the soccer field.
- Other factors: Such as sleep, nutrition and body weight management.

This article describes many different ways in how the McKenzie method can be applied more effectively in my humble opinion. As always, thanks for reading!
Want to learn more about exercise and pain?
Ben Cormack has done a Masterclass lecture series for us on:
“Exercise and pain: exploring a complex relationship”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Leave a comment (2)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
You can’t have authority in a system if you have not completed the required post graduate education to a level recognised by the governing body, here the McKenzie Institute.
To have qualifications that demonstrate your competence in the McKenzie Method you need to have completed all 4 courses and then passed either Credential Exams at a minimum, or the 10 week clinical program the be a Diplomat.
To suggest a knowledge of any depth in the McKenzie approach by reading free online content or a few blogs is ludicrous.
This was recognised and published by Ron Donelson in his commentary in Spine Journal.
McKenzie method is not to fix it , is to understand the problem to help further with proper management that depends on classification to certain categories. If you not at least , went through full training with certain method or certified in the method don’t play with modification please. The latter might bring more modification to your perception of the method not the method itself. Henryk Kielsznia Cert. MDT