
Over the past year, as my commute to and from work has increased, I’ve taken advantage of this time to listen to more podcasts pertaining to Physiotherapy and Strength and Conditioning (S&C). The most thought provoking podcast was by Mike Reinold, who discussed the concept of outcome measures (1). The main question that stood out was:
“Are we measuring what’s important to the patient or are we doing outcome measures just for the sake of doing them?”
This was followed up by “how can we measure our patients goals in a thorough, yet efficient way?” In this article, I discuss how to better fit outcome measures to patient goals.
But first, let’s get the obvious out of the way.
Yes, for certain situations (e.g. workers compensation and motor vehicle insurance), jurisdictions and insurance systems (such as in the US) you may need to have specific outcome measures to get reimbursed for your services. That is the nature of dealing with insurance. But for most cases, are we doing outcome measures to assess what’s important or just for the sake of doing them?
I would argue in a lot of cases it’s more the latter. Don’t get me wrong, questionnaires have a time and place. However, I find in a lot of cases patients don’t understand them, fill them out incorrectly, and/or get unhappy by feeling bombarded with a ton of questions that may not be relevant to them. Plus, not gonna lie, it can be very annoying when you have an assessment start 10-20 minutes late (or even later) because of a client struggling to get through questionnaires.

A Different Approach
I like to let my patient’s history and goals guide which outcome measures I use and then administer them. These days there are so many technological options to send questionnaires (if needed) that patients can complete them on their own time. Or worse comes to worse, you send them a hard copy that they bring back the next day or send to you via scan, fax, or phone picture.
Admittedly, other than motor vehicle and workers’ compensation scenarios, I don’t use a ton of questionnaires in musculoskeletal physiotherapy, outside of the Patient Specific Functional Scale (PSFS). I got the idea from the aforementioned podcast and use the PSFS for goals a patient is working towards (i.e. squatting, kneeling, walking, running, working overhead), and (if possible) observe the patient doing those tasks. Then I will re-administer the PSFS periodically as needed.
Other Outcome Measures
Pain
Pain is pretty straightforward to measure and can be done via the Numeric Pain Rating Scale or the Visual Analog Scale. That said – pain goals need to be realistic and shouldn’t be the only focus of therapy.
Range of motion
Range of motion (ROM) measurement is again pretty straightforward. In most cases, if ROM is a goal and/or the client is post-fracture, surgery, or dislocation; I’ll measure ROM during every appointment.
Tolerance to ADLs / physical activities
You can look at self-reported patient tolerance for how long he/she can do a desired task (e.g. gardening, walking, running). Let’s face it – doing a 1 hour walk or run test isn’t feasible in most clinical settings. For clients who have limited walking/running function you can look at:
- Walking: Two minute or six minute walk test
- Gait speed: Timed Up and Go or gait speed test. Two minute walk test can also be useful in this regard.
- Running: Run Tolerance Test – this consists of getting the client to run for 5-10 minutes on a treadmill (depending on your setting and situation) and tracking how long they can go for before experiencing pain or fatigue. Thanks to Tom Goom aka ‘The Running Physio’ for teaching me this one.

Strength
Strength is a trickier one as research has debated the reliability and validity (2, 3) of manual muscle testing (MMT). Don’t get me wrong – I still like MMT to see if there’s a glaring weakness between sides or pain with resisted contraction, but beyond that there are a lot of issues. Most notably, it is a highly subjective test that can be affected by a bunch of different things including positioning, effort/force used by the tester, and our subjective bias towards measures that prove what we are doing is working.
Some people use dynamometers in conjunction with MMT but I have never used these before (outside of the Jamar Dynamometer for grip) and can’t comment on them. Beyond a glaring side to side difference in strength, for clients who have put strength improvements as a goal, I like to use the following strength/capacity tests (in no particular order).
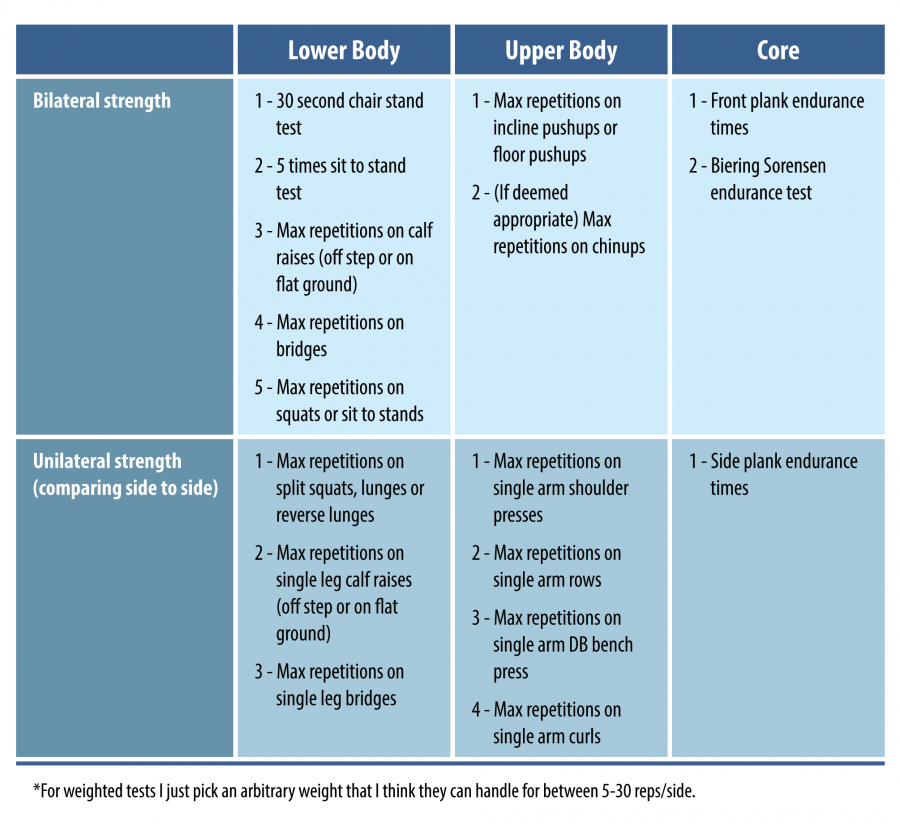
You certainly don’t have to do these or be limited to these outcome measures. But, if you’re someone who doesn’t have fancy testing or exercise equipment (i.e. dynamometers), these can be useful, straightforward and objective ways to track strength improvements in clients.
Balance
When it comes to balance, I quite often see clinicians go one way or the other. Either clinicians assess balance very briefly and just get someone to stand on one leg and move on. Or, clinicians put clients through a dozen different balance assessments.
Balance assessment is important but shouldn’t take all day either. I generally like to use the following:
- Static balance:
- For most clients I use a combination of single leg stance and the Modified Clinical Test of Sensory Interaction in Balance (mCTSIB).
- I sometimes use the Balance Error Scoring System (BESS) test for athletic clientele or clients who may have deficits with higher level balance/stability activities that need addressing.
- Dynamic balance:
- I use the Dynamic Gait Index to assess dynamic balance and mobility. I put more stock on this score than on the static balance testing in most individuals. Really, how often do you need to stand on one leg on a foam mat with your eyes closed?
Unless you’re working with a client who’s really deconditioned or has significant post-concussive symptoms this should take less than 10 minutes to do.
I am also a big fan of the Berg Balance Scale. However, almost all of it can be covered by the above tests and by thoroughly observing the client during sitting, standing, transfers and gait. Plus, I like the longer static balance testing times on the above mentioned tests in comparison to the Berg Balance Scale.
Specific goals
Another simple way to look at measuring outcomes is whether or not a client achieved their specific goals or not. This should be broken down into 3 categories: fully achieved, partially achieved (i.e. the client made progress but did not achieve his/her full goal), and not achieved at all (i.e. no progress or even regression).
Do You Even Use Questionnaires?
I believe there is a time and place for the traditional questionnaires (e.g. Lower Extremity Functional Scale [LEFS]) when there are a large number of functional limitations and goals that the client has. These should be administered after the assessment, not before. It doesn’t make sense to give a LEFS to a client who only has pain or difficulty in the 4th quarter of a basketball game or to a client who’s just had ACL surgery and is on crutches. Fundamentally, the hassle of going through a questionnaire, for both you and the patient, has to be worth it for the information gained and its impact on management.
What About Risk Factor Screening Questionnaires?
The Tampa Scale of Kinesiophobia has certainly been scrutinized in the literature (4, 5). I like both the Keele Start Back and the Orebro Musculoskeletal Pain Questionnaires. However, they are designed to predict who does/doesn’t develop persistent pain so their use can be limited if the majority of your clients have had pain for >3 months. I also like the Fear Avoidance Beliefs Questionnaire, although it is more specific to clients who have had an injury at work and/or are off work because of pain.
Wrap-Up
This blog may sound like I’m putting a complete bash on outcome measure questionnaires. That isn’t the case. The goals of the article were to:
- Make you rethink which outcome measures you use and when.
- Give you some different ideas on how to measure outcomes for your patients.
- Provide guidance on different (and potentially more efficient / effective) ways to administer the outcome measures you already use.
Are there any other ways you measure the progress of your clients? If so, drop a comment below or send me a DM. As always – thanks for reading!
Want to master behaviour change?
Dr Serena Simmons has done a Masterclass lecture series for us!
“Behaviour Change in Clinical Practice: A Physio’s Guide to Psychology”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!