Measure what matters: Mastering serial testing in chronic pain

In this blog I will present a framework for systematising and building value in your objective assessments for people with chronic pain. I have been thoroughly enjoying re-entering this space lately as a more senior clinician with a specialist coaching and strength and conditioning skillset. I have spoken to the challenges most clinicians face when managing chronic pain before in this blog on the RESTORE trial – this too, reflected my previous daunting experiences with treating chronic pain.
Due to the limited time and resources, chronic pain sufferers often don’t get the thorough systems thinking that our athletes enjoy. So this framework is my attempt to help clinicians struggling in this space. And here it is in four words… Master your serial testing!
Background
Before we go too deep – what is this “serial testing” you speak of? Basically, it’s the repeated testing and tracking of objective markers through time. Sports medicine and performance clinicians will be very familiar with this. A great example is the quadriceps strength testing completed at multiple intervals across the course of an Anterior Cruciate Ligament (ACL) rehabilitation program to help determine next steps (1, 2).
However, I feel that chronic pain can be slightly more daunting, since pain, strength and function often aren’t as well correlated (3). For this reason, I have developed this three-factor venn diagram to explore how to choose and frame your serial testing with your chronic pain patients. We will also be exploring how this model improves patient buy-in through the Theory of Consumer Values (TCV) (4). Applying the TCV isn’t aimed toward “selling your service”, but instead providing a service that people will value, which is super important, especially in chronic pain!
The TCV is split into 5 Parts – FECSE:
- Functional: Relates to meeting the needs of the patient in their context (how you can help them in their life)
- Emotive: Relates to the experience of accessing the service (clinician soft skills and interactions, understanding and empathy, environmental connotations)
- Conditional: The cost-benefit analysis of the service. Even if it meets a functional demand, is it worth the resources (monetary, time-cost, opportunity cost) required to access?
- Social: I think of this as your “street cred’”, or your reputation as a service, and then also your ability to create that sense of belonging/relatedness required as outlined in motivational theories
- Epistemological: Does your service spark the inquiry impulse of learning in the patient? (5) Are they coming in because something in the service makes them innately curious? E.g. “I wonder what my test will show this week”
Ok, that’s the TCV explained, now show me the model…
The chronic pain serial testing model
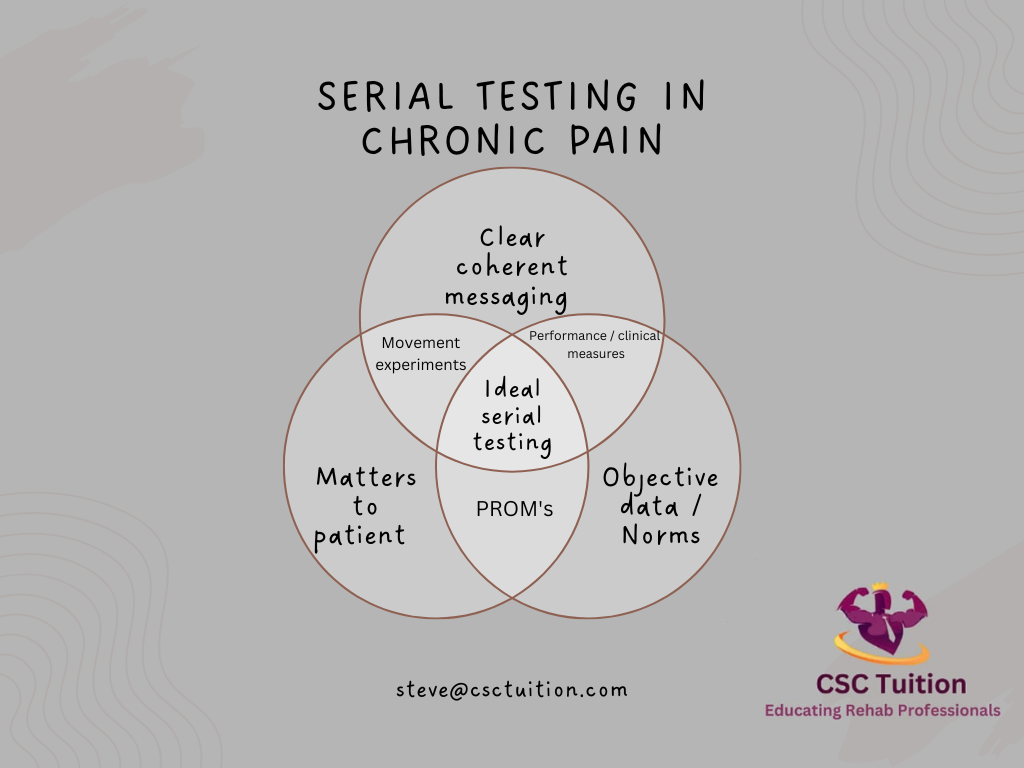
This model breaks our testing choices down into three distinct but overlapping circles that we can decide to test and track over time. The serial testing sweetspot exists where all these circles meet. But.. Let’s first break each down before we put them together:
Circle 1 – What matters to the patient
To some degree testing must be relevant to the goals or concerns of the person seeking care. The main aspects of the TCV model this targets are the “functional, emotional, and conditional” perceptions of value. Ensuring this circle is considered in a serial testing battery demonstrates empathy, and an understanding of the importance of costs versus benefits of your service in the patient’s journey. Giving them things they can track at home as a proxy for your serial testing is good practice to avoid reliance (6).
Circle 2 – Clear and coherent messaging
This one may not be as intuitive. This directly relates to the social, epistemological and emotive sections. The tests that you chose through shared decision making should ideally not be contradictory to any narratives you believe would be best to facilitate patient recovery (e.g. telling someone “their back is strong” but then being too afraid of flare ups to include any direct measures of back strength). This type of contradictory message could undermine that social/street cred’ aspect. Further, clear and coherent messaging should spark curiosity in our patients around how their results fit into the broader narrative of recovery.
NB: Here we can frame our testing in two main ways:
1 – Validation of the patient experience. E.g. “yes this is your safe limit currently, so we probably shouldn’t exceed it often”.
2 – Expectancy violation: The way you perform the tests forces them to confront their negative beliefs. E.g. getting the patient to guess the result of a test (usually they will anchor low), then showing them the actual results (often with surprise regarding how they exceeded their expectations) (7).
Circle 3 – Objective data/norms
This is the bread and butter of clinical/performance testing. This is the ability to choose tests that have strong reliability and repeatability, give objective data that can be tracked over time, ideally with Minimally Clinical Important Differences (MCIDs), and have normative comparisons. Nailing this is not only being clinician centric, but we can also utilise this to facilitate the functional and epistemological values of the patient so the data means something to them in their lives (8, 9).
Here I’ll flesh out these concepts slightly more with a common back pain example.
NB: If there isn’t one test that meets all domains, having a few that meet more than one domain added together is a good second place.
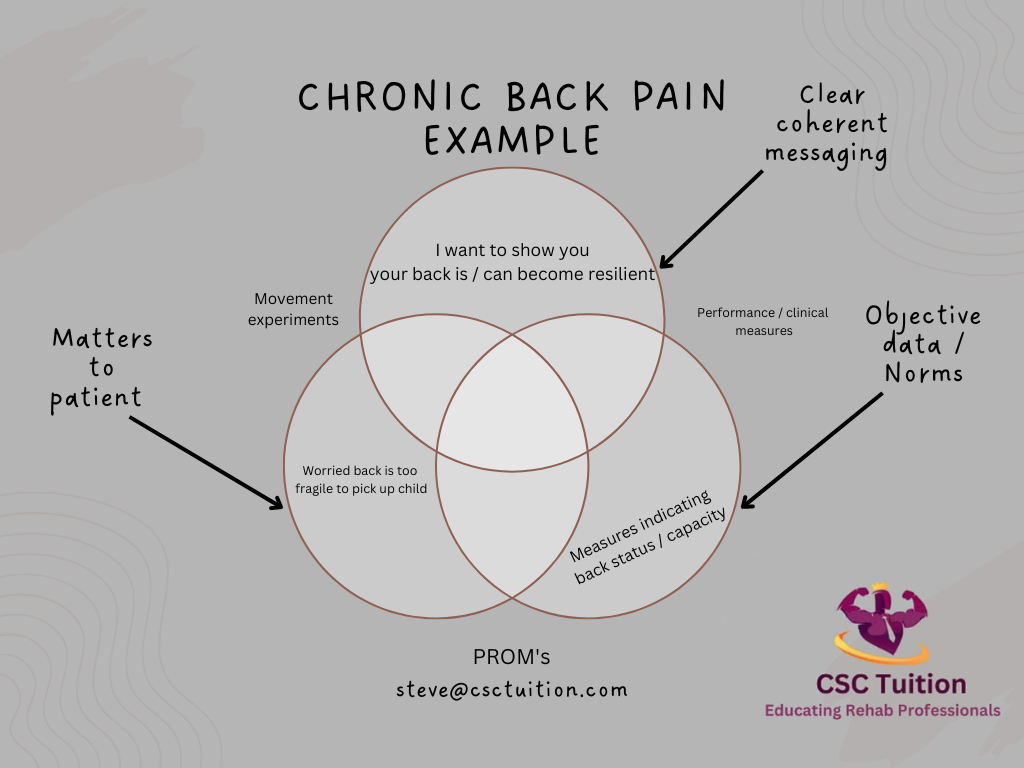
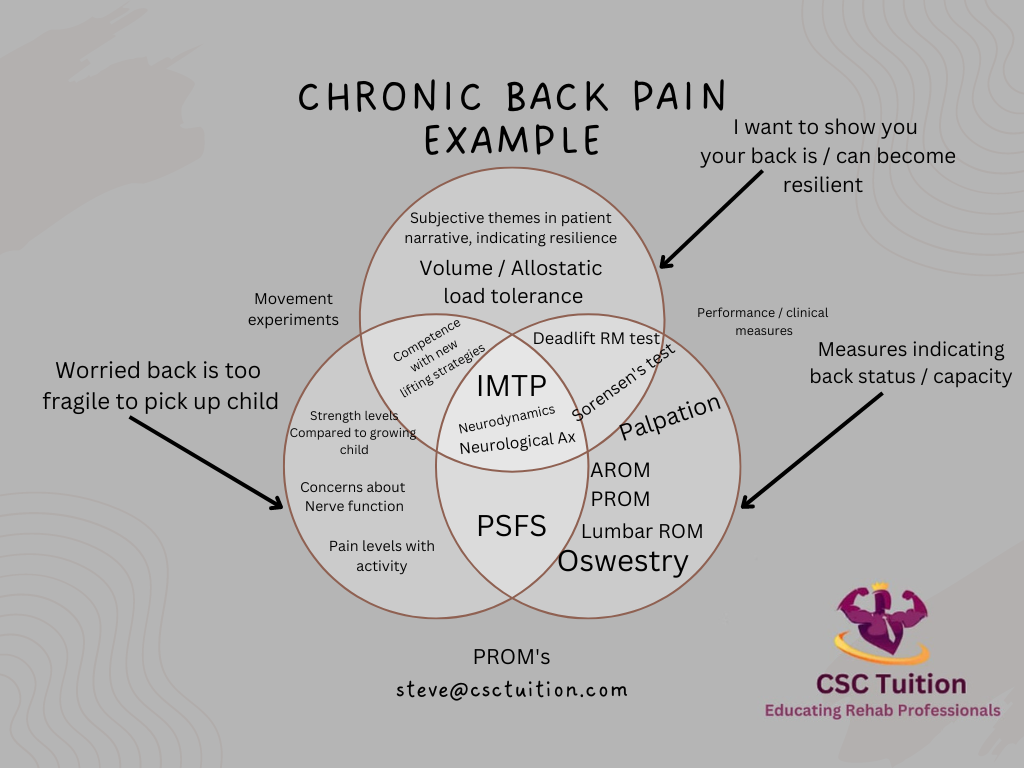
Here we had someone who was worried that their back was too fragile to pick up their child and doing so would “damage their nerves”. In this case an example of a clear and coherent message is that their “back is resilient!”. To do this we chose some pertinent tests with the patient to help us determine how resilient their back is over time. These tests have normative or repeatable objective data that can help allay patient concerns and help them learn about their condition.
Here we have chosen together our testing battery to be the Isometric Mid Thigh Pull (IMTP), the Straight Leg Raise (SLR), and a lumbar spine neurological exam including dynamometry and reflexes. Together with the patient you will agree on a rough serial testing schedule for these measures.
This video shows a discussion of how this conversation might go:
Sticking roughly to these testing schedules can be an important step in helping the patient learn about the things that impact their function and condition. It is important to not get stuck on any one data point, but rather the trend. Individual testing sessions are instead great ways to educate how the effects of chronic pain can fluctuate along with the patient’s current allostatic load (10).
Wrapping up
So there we have it. Hopefully this three factor model of serial testing can help you get confident in delivering a service that people in chronic pain will really value.
If you want to learn more about chronic pain management from the experts, watch Mike Stewart’s Practical Guide to Persistent Pain Therapy Masterclass now!
Want to learn more about communicating with patients?
Mike Stewart has done a Masterclass lecture series for us on:
“Know Pain: A Practical Guide to Persistent Pain Therapy”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!