Clinical Pearls on Tendinopathy from Dr Jill Cook

We know that tendons love load, and tendinopathies need load for effective rehab.
But where do we start?
What type of load?
And when is the load too much?
In this short blog, we’ll highlight the key points from Dr. Jill Cook’s episode – “Clinical Pearls on Tendinopathy” – on the Physio Explained podcast (where you can learn from the best in 20 minutes or less). By the end of the blog you’ll have hopefully learned some immediate strategies to implement with all of your tendinopathy patients for more effective patient outcomes.
Step 1: Determine the starting point
We know that tendon pain and functional capacity aren’t related to pathology. Some patients present with pain but have minimal pathological findings, while imaging people without pain can also show degenerative changes. Therefore, it’s important to note that imaging shouldn’t change our clinical prescription. Instead, we should focus on using a thorough history and physical examination to identify the tendon’s current capacity and determine our clinical starting point.
Step 2: Identify the tendinopathy type
- Reactive tendons (rarely seen in clinics)
Clinical findings:
- Young individuals
- Acute overload
- No prior history
- Degenerative (or reactive on degenerative) tendons
This accounts for almost all clinical presentations.
Clinical findings:
- Often a small but recognisable load increase caused the pain
- Mostly middle age and older adults
- Tendons are dysfunctional (likely sedentary or low activity) prior to presentation
What They Need: Loading!
Step 3: Where to start with tendon loading?
Tendons have a high capacity to tolerate loads. However, when the demand exceeds the current tendon tolerance (by often adding too much too soon), degenerative tendons become symptomatic and present clinically.
Where we start tendon loading is incredibly important (and should be based on their current functional capacities).
This 4 Stage Continuum starts at the very unloaded beginner and builds for the very loaded runner. Note that we shouldn’t always be starting at stage one. It’s important to determine the functional capacity of the tendon and start there, with the goal being to move up the continuum as tolerated.
- Isometrics (for pain and motor control)
E.g. Challenging isometrics (≥ 75% MVIC) - Heavy Slow Resistance (HSR) (for tendon stiffness and muscle strength above and below the musculo-tendinous unit (MTU))
E.g. ~8 reps per set at 8/10 difficulty (2 reps left in the tank) - Plyometrics (if required for their activities)
E.g. Jumps and hops - Faster Loads (if returning to running activities)
E.g. Stair running and skipping, change of direction
Depending on the activities the patient wishes to return to will also determine which stage completes the tendon rehabilitation journey.
For example, a sedentary older adult whose goal is to continue walking without pain may complete stage two and only perform only some exercises within stage three. Conversely, a field sport athlete will be required to complete stage four if they are to return to running. The final stage should align with replicating the activities they wish to return to.
When identifying a starting point, it can be helpful to remember that slow loads are not high tendon loads, and are also rarely provocative. Starting with HSR is therefore a great option for most tendinopathies as the muscle will fail prior to the tendon, yet it allows for tendon stiffness and muscular strength to be built.
Step 4: When is the load too much?
Tendons tend to improve with activity and worsen the following day. Hence why it’s critical to track 24 hour post loading symptoms.
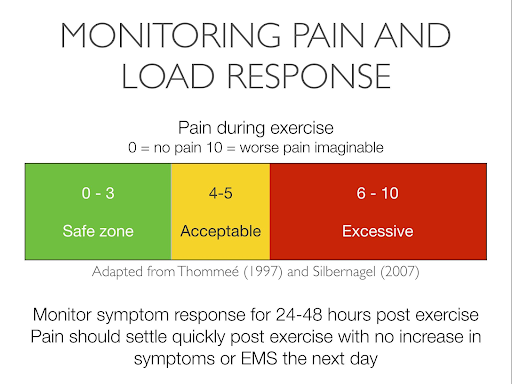
Figure 1
While the tendon pain scale can be a good guide, it’s incredibly subjective and provides no real definitive answers for clinicians or their patients.
As a much simpler version to patient education, we can instead use this:
If you are worse tomorrow, you’ve done too much.
It’s also helpful to note that quicker loads (think stage three and four using plyometrics and running drills, respectively) are much more likely to aggravate reactive on degenerative tendons. An aggravation, determined as an increase in symptoms either during or the day following exercise, is a tendon that isn’t tolerating the load continuum. In these instances, reduce the load and try again.
Wrapping up
- Tendons can be frustrating to manage, especially when loads aren’t consistent.If symptoms increase following exercise therapy, it’s important to reduce loads. Rarely should we be recommending complete rest. This often does more harm than good and delays the rehabilitation process.
- Don’t fall into the trap of underloading tendons (especially in stage one and two).There is such a small likelihood of provoking a tendon in these stages, that we really need to both educate our patients around the benefits of this and ensure we are really challenging the musculotendinous unit to strengthen under load.
- Don’t forget to address dysfunction.If a tendon is degenerative, look at what the underlying causes of this might be. Tendons cannot be treated in isolation.
For deeper, evidence-based instruction beyond the podcast, check out our Managing Lower Limb Tendinopathy Masterclass. Get expert guidance and earn CPD/CEUs while you learn in this two hour course.
🎙️ Learn from the best in 20 minutes or less
💡 Our podcast ‘Physio Explained’ takes you inside the minds of the brightest physios in the world.
🎧 You won’t find an easier way to learn on the go.

Don’t forget to share this blog!
Leave a comment (1)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
powerful!