
In Neil’s commentary, he keenly evaluates the clinical decision making from gathering evidence from a wider perspective and applies it to the particular case. He also delves into the clinical acumen required for sense-making for both the therapist and the patient. I would like to discuss multi-factorial reasoning and move towards thinking about dispositions. In writing my paper the most difficult task was conveying the difference between a multifactorial causal approach and a dispositional causal approach
There is a growing sense of recognising the multi-dimensional nature of clinical encounters where the utility of a whole person approach far surpasses unidimensional approaches (O’Sullivan et al, 2016). A significant challenge to a whole person approach, despite it being grounded in common sense and resulting in improved clinical outcomes, is that when seeing a person who presents with a clinical problem, once all the evidence is gathered, by whatever means, how do we make sense of it and what do we do about it? One way to develop a multi-factorial model of explanation, quite simply, is to consider a number of categories and start to fill in these areas with data. An example might be using a biopsychosocial approach, whereby biomedical, psychological and social profiles are developed with the information gathered by the history and physical examination. Each of these areas aim to move away from biomedical reductionism (Engel, 1977) but in its place lies biomedical, psychological and social reductionism. But we have to start somewhere, do we not?
Jones, Edwards and Gifford (2002) present a classic paper applying the biopsychosocial theory to clinical practice. They refer to Gifford’s mature organism model and to Jones’ hypothesis categories, as well as to the interpretive and insightful understanding of Edwards, to provide a great person centred approach. This culminates in an excellent reasoning model providing epistemic (knowledge based) and therapeutic value. The paper pays attention to both the empirico/analytical approach, such as the generation of hypothesis categories, and also to an interpretive methodology such as the way in which the categories relate to each other.
Using a multi-factorial method certainly has its advantages and appears to embrace a holistic approach. By that I mean, identifying all the potential factors that are present to the complaint and addressing them, in turn or together, to create a critical change in the condition resulting in a positive or desirable effect (figure 1). However, how many times do we think we have addressed this and yet no change has happened? How disappointed are the people in our care when they have worked hard with the management plan with no change? We might have thought that the causal mechanisms of the disorder would have been ameliorated, according to the model we agree with and find most compelling!
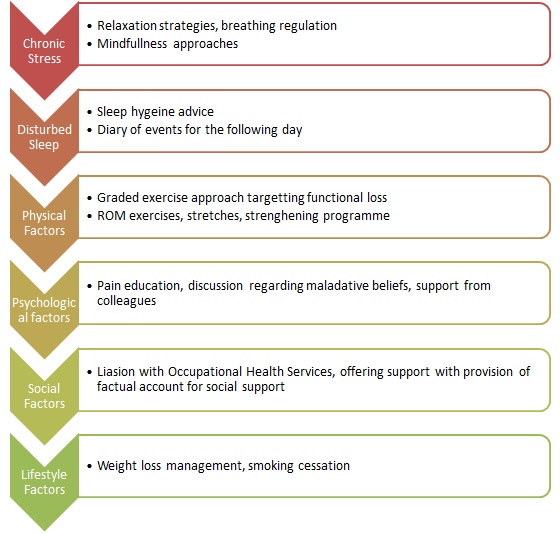
Figure 1: An example of using a multi-factorial treatment and management approach
Van Ravenzwaaij et al (2010) described a number of explanatory models from the literature that may shed light on symptoms that we have no clear explanation for. These include physical explanations (immune system sensitisation theory, endocrine dysregulation theory, autonomic nervous system dysfunction theory and abnormal proprioception theory), psychological explanations (somatosensory amplification theory, sensitivity theory) and hybrid explanations (sensitisation theory, signal filter theory and an illness behaviour model). Surely, by using a multi-factorial model it would not matter what causal mechanism(s) could explain the condition, treatment or the management. But by addressing all the identifiable factors would have had some effect on at least some of those proposed theories….surely!
Perhaps we should examine the underlying metaphysical theory (ontological) explanation as it might be more favourable to consider that certain powers may interrupt, counteract or simply overpower (overdispose) others so that no effect takes place. Erikson et al (2013)in their perceptive paper examine beneath the surface of the complexity that we face every day and is certainly worth a read (maybe a few!). This dispositional perspective examines the causal components at a deeper level. Please consider this paragraph:
To move from monocausality to multifactorial causation does not in itself guarantee that we take the complexity seriously. If our methods are designed to treat each factor separately, the phenomenon as a whole is lost even if we include many factors and add them up. Complexity is a core idea of dispositionalism, and this is particularly clear in causation. All actual effects will be multifactorial. The flammability of a match is not alone sufficient for it to light when struck. It will also require the presence of oxygen and reasonably arid conditions. Given that all such factors contribute, and all such may be hypersensitive in relation to what they manifest, then the medical uniqueness of each patient starts to look a credible possibility. Understanding causal interaction is not only about taking into account all the factors involved and how they compose. It is also a question of magnitude or degree. On dispositionalism causes and effects come in degrees. They are not a matter of “all or nothing”.
Multi-factorial thinking is not enough! In my paper, I attempt to describe how a dispositional approach might be a step forwards with the use of the vector model (figure 2). The vector model describes how causation may work and be a significant contributor to clinical reasoning. Further work in progress!

Figure 2: The Vector Model (Anjum and Mumford – Getting Causes From Powers)
One of the key advantages of a dispositional approach verses a multi-factorial approach is the attention to context sensitivity and non-linearity. For example, exercise has been shown to be beneficial for chronic musculoskeletal conditions, including exercising into pain compared to pain free exercises, certainly in the short term. However, the adherence and compliance of exercising into pain may be a barrier to the treatment effect. This is demonstrated, to an extent, by the relatively high attrition rates identified within studies and also the exclusion of widespread pain disorders such as fibromyalgia. A multi-factorial approach will use exercise as a treatment but the context of when and how it is applied may not be taken into account, including the potential for exercise to have a deleterious effect. The presence of causal factors that dispose an individual towards having reduced descending noxious inhibitory control mechanisms (e.g. poor sleep, chronic stress, anxiety and depression) have variable outcomes to exercise including making symptoms worse therefore reducing adherence to an evidence based treatment. A dispositional account recognises the individual context and may focus treatment towards the factors that are reducing the inhibitory control mechanisms prior to exercise prescription. Later, a graded exercise programme may be more successful, both in terms of adherence and treatment effect. This is just one example of a well-intended treatment modality resulting in a non-desirable or negative outcome using a multifactorial approach. Emergent phenomena, such as the manifestation of persistent pain, do not follow linear paths bereft of context and a dispositional approach may prove fruitful.
This was originally posted on Matthew Low’s website. You can click here to read more blogs from them.
👩⚕️ Want an easier way to develop your assessment & treatment skills?
🙌 Our Practical video sessions are the perfect solution!
🎥 They allow you to see exactly how top experts assess and treat specific conditions.
💪 So you can become a better clinician, faster.

Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!