The Two Most Common Misconceptions about the FMS

Over the past three years as part of my PhD, I’ve been researching the relationship between movement and injury. A recent Twitter discussion reminded me that people on either side of the great FMS social media debate are still confused. I figured I’d put my research efforts to good use to clear up a couple of common misconceptions.
Misconception #1: The FMS composite score can predict injury.
When the FMS first became popular in the late 2000s, its creators touted it as an injury prediction tool [1,2]. The trouble was, at the time they had zero scientific evidence to back that claim up.
It turns out scoring low on the FMS does increase a person’s risk of injury slightly [3,4], but it doesn’t guarantee it. In other words, while low scores are associated with injury, the FMS does not predict injury on an individual basis. Big difference [5].
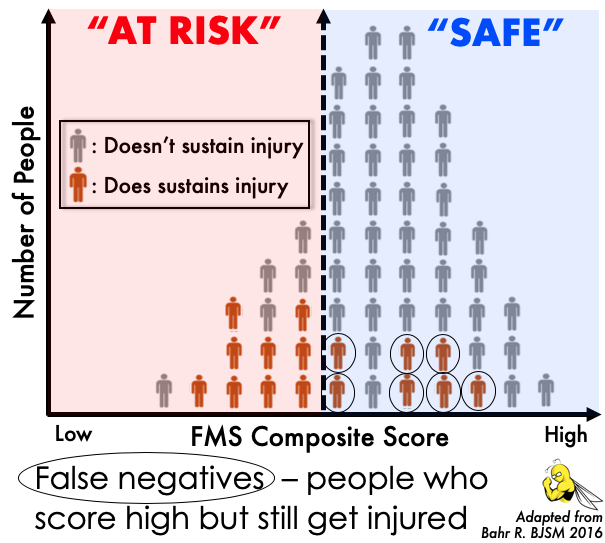
Specifically, when the FMS is conducted on a large group of people, as in a scientific study, we tend to see a lot of false negatives (people who score high but still get injured).
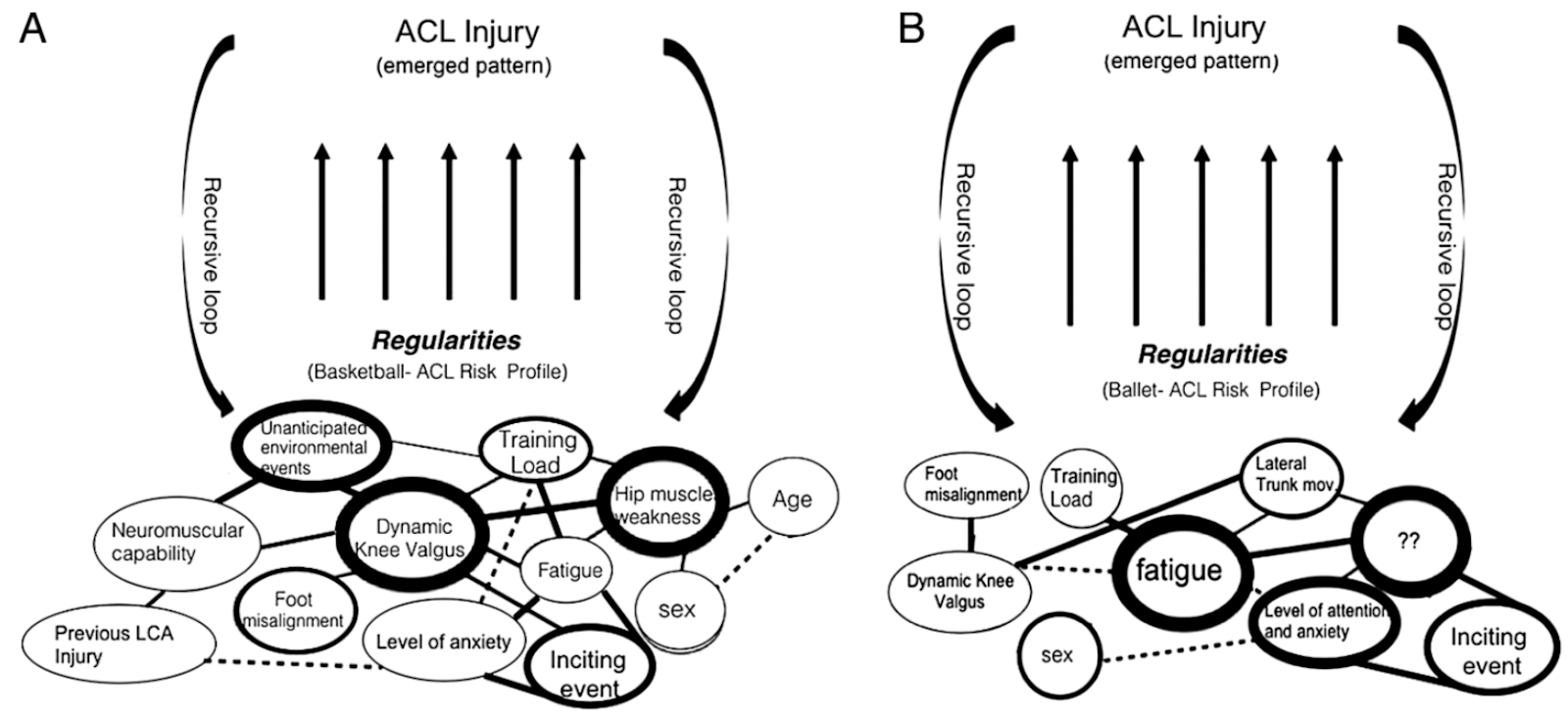
The fact that the FMS can’t predict injury actually isn’t that surprising. There’s no one thing that predicts injury [6]. This is because injuries aren’t caused by just one factor. Instead, they’re the result of a complicated web of interrelating factors — a web that’s different for every person based on the types of activities they do [7].
Misconception #2: Since the FMS doesn’t predict injury, it’s useless.
As the evidence against FMS for injury prediction mounted, its creators quietly walked back their initial claims. Understandably, many evidence-based professionals take issue with the way the FMS folks handled their business. No doubt, they put the marketing cart before the science horse.
Nowadays, the FMS team talks about the purpose of the screen being to rate movement quality/competency [8,9]. In particular, the FMS looks for movements a person can’t perform or that cause pain. Most would agree this is a reasonable approach when working with someone for the first time.
Obviously, movement professionals were scrutinizing movement long before the FMS came along. What the FMS did was systematize this process using seven bodyweight tests and standardized scoring criteria for each.
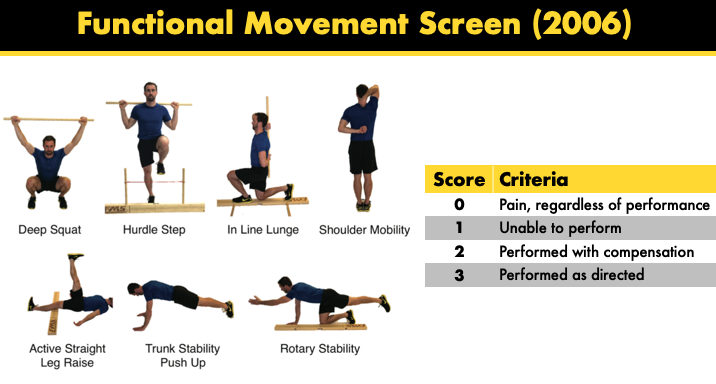
The whole thing takes about 10 minutes and provides quick and dirty information about a person’s mobility, motor control, and symmetry — all of which can be used to guide exercise selection [10]. Hardly controversial when used in that way… right?
Well, there are a couple of important limitations. First, the seven tests are somewhat arbitrary. They’re only a small subset of the movements humans are capable of. Moreover, testing at slow speeds with bodyweight only isn’t indicative of how a person will move at faster speeds, with added load, or under fatigue [11].
The other issue is that the FMS relies on the notion that some ways to move are better than others. This is controversial, to say the least. We know for example that people differ anatomically (e.g. bone structure, limb length ratios, muscle insertion points), and these differences affect movement strategies.
Unless something’s a known mechanism of injury, it’s difficult to state with certainty that it’s “dysfunctional.” Granted, it’s a common misconception that the FMS demands “perfection.” In reality, the FMS asks only for “good enough” (i.e. they allow some wiggle room away from their ideal performance on each test).

So is the FMS useless? No. It’s simply a lens to view movement through. Do we need it to tell us, for instance, not to put a bar on a person’s back who can’t squat with just their bodyweight? No again. It’s just one example of a standard operating procedure.
Most movement professionals worth their salt should be able to put together their own assessment that:
- Is specific to their setting and the population they work with
- Includes added speed, load, and fatigue (when appropriate) to create a comprehensive movement profile
- Includes additional “breakout testing” depending on what the initial tests show to dig deeper into movements that appear limited
- Helps them select exercises that are appropriate to the trainee’s level and goals
Sample breakout tests for a squat
Chances are good your assessment will have some sort of squat, some sort of push-up, some sort of look at hip and shoulder mobility, core stability, etc. [12]. Perhaps to the specifications of the FMS or not.
The FMS is by no means perfect. Use it or don’t use it, but for goodness’ sake, do something to systematically assess movement. Don’t just guess.
This was originally posted on Travis Pollen’s website. You can click here to read more blogs from him.
Want to learn more about cancer rehab?
Germain Tan has done a Masterclass lecture series for us!
“Cancer Rehabilitation Essentials: A Practical Guide for Physiotherapists”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Leave a comment (2)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Relatively neutral view…
However, the clarifications given favouring movement screen and concluding remark of assess movement systematically is ambiguous.. this is very vital as every assessment must lead to effective management , if that’s not possible what’s the role of assessment.. in short, if my systematic assessment of functional movement says the movement is not good enough, what should I do ? Force the pt to perform in good enough way ?
@sheikabdulkhadira.m.k. I think maybe ask the patient if this testing mouvement causes symptoms or decreases it. Then find the way to use it for therapy. I think it was J. Lewis who said “your test become your treatment” assessing a shoulder.