
Mobilization, manipulation, dry needling, massage, myofascial release, Gua Sha, Jones Strain-Counterstrain, fascial stretch therapy, instrument-assisted soft tissue, active release, effleurage, scraping, etc. There are so many different types of manual therapy it can make your head spin, give you anxiety about your lack of expertise, and rob your piggy bank blind on the quest to learn them all. Each one of these manual therapies tend to focus on varying tissue issues and many often boast their own special secret to treating dysfunction in the musculoskeletal system.
Some of these techniques were taught to you in school, while some are “higher level” techniques. Some are even trademarked and only taught to you once you have reached a certain level of experience. It’s not uncommon to see the purveyors of many of these manual therapy approaches claim that their technique could solve the problems for all those stubborn patients who just won’t get better.
There’s no doubt that manual therapy is an appealing topic and valued skill set in most of the physical medicine world. The ability to lay your hands on someone in pain and make short-term changes that help them feel better has an incredibly powerful appeal to it. Each one of us in the physical medicine space want nothing more than to help those patients in front of us get out of pain and get back to the activities that make their life enjoyable. The big question lies in what is actually happening during this manual therapy interaction, and whether or not that technique you are performing is actually doing what you say it is. So, what is it that manual therapy can and can’t do?
The Can’ts
- Accurately and reliably palpate for positional and movement faults:
- Bahram Jam and company did a nice write up on this topic with several sources cited (1)
- Accurately and reliably determine which tissue “is the cause of pain”:
- Pain is much more complex than what is going on at the tissue level. If that isn’t good enough then read these two books – Explain Pain and Making Sense of Pain
- Lengthen / stretch out / deform connective tissues like muscles, tendons, ligaments, and fascia:
- Plenty of data to show that even with aggressive stretching for weeks/months it is VERY difficult, if not darn near impossible, to change muscle length or contractures in adults (2, 3, 4, 5)
- Solid evidence here to demonstrate how incredibly strong our connective tissues are (6, 7, 8, 9, 10, 11)
- “Release” muscles:
- What does it even mean to release a muscle? Is this a change in length? Is it a change in neural tone? We have to first define and agree upon what “release” is before we can reliably study it. Once we agree on what it is, we have to determine a valid measure that can give us reliable data on if we can or cannot cause a change. Until then, we are just using therapy jargon that has no real meaning.
- Put joints back in place:
- Ok….yes…we can manually relocate dislocated joints. However, this is more along the lines of the vertebral subluxation model that has yet to be proven after over 100 years, and the all too common physical therapist/osteopathic concepts of a ‘stuck rib’ and rotated pelvis due to the SI joint being “out”. You can check out a 30 minute video I did on the topic of assessing and “correcting” the SI joint here.
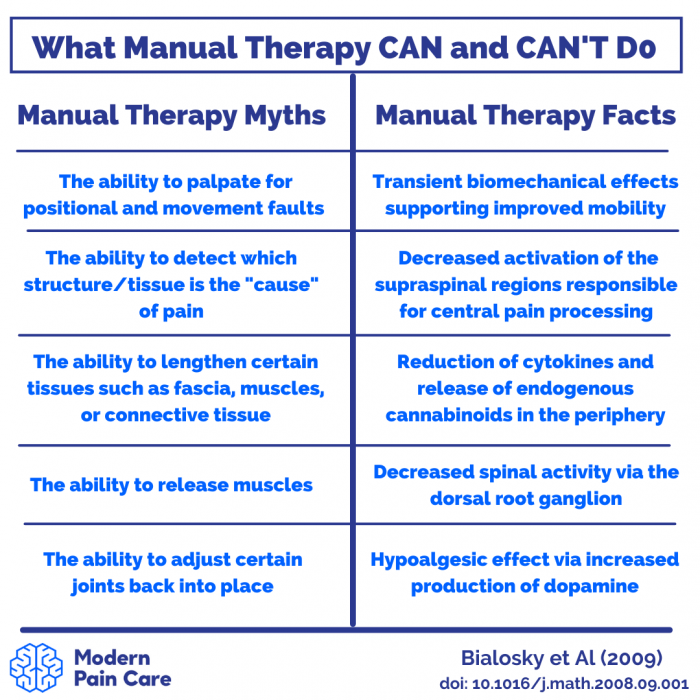
Image credit to Cameron Faller from Modern Pain Care
The Cans
- Induce transient peripheral biomechanical effects:
- This mainly comes back to the fact that you actually need to apply a mechanical force to initiate the chain of neurophysiological responses which produce the outcomes associated with manual therapy.
- Theoretically, we may be able to induce a temporary reduction in the sensitivity of peripheral mechanoreceptors through the use of light physical touch.
- Temporarily increase ROM and decrease pain by altering the ascension of nociception up the spinal cord/brain:
- Put simply, this is gate control theory, first proposed by Melzack and Wall here.
- There’s nothing fancy about it. If you whack your shin on the coffee table and immediately reach down to rub it and it feels a bit better, you’ve done effective manual therapy and caused interneuron gating at the dorsal horn of the spinal cord.
- In some cases, there may be significant perceived value in temporarily reducing a person’s pain to allow more comfortable participation in exercise, proving to the patient their pain is modifiable, and opening up the floor for discussion on tissue sensitivity vs tissue damage.
- Improve therapeutic alliance and help build rapport with the patient:
- Manual therapy certainly is not necessary to build patient rapport or bolster therapeutic alliance. However, manual therapy tends to provide some short-term pain relief (as mentioned above) which can increase the patient’s confidence in the therapist as well as their own ability to get better.
- Furthermore, at present, there is a widespread cultural belief that manual therapy is helpful.
- Taking into account patient preferences and expectations, as well as the “human social grooming effect”, physical contact between people in an intimate and trusting healthcare environment can often be a beneficial way to create alliance, confidence, and understanding.
- Alter activation of supraspinal regions critically involved in the human pain experience:
- This sounds fancy really, but is actually just a part of the placebo effect, or meaning response as it is now becoming known (12, 13, 14).
- A strong ethical argument can be made in favor of leveraging all non-specific and indirect aspects of the patient-clinician interaction to maximize the possibility of a more robust treatment effect when targeting subjective experiences such as pain.
This list certainly isn’t an all-encompassing account of every possible way in which manual therapy can and can’t exert an effect and influence pain. Realistically, several of these aspects may play only a very minor role in pain modulation, and there are likely many more mechanisms in which manual therapy may impart a change to the dynamic system of a human being experiencing pain and embedded within a specific environment that we have yet to discover or measure with well-designed studies.
Try to avoid hearing what I’m NOT saying. I am not attempting to say that one should no longer use manual therapy in their practice, as it does consistently show to have some small effects and is often an expectation within many people’s care (read a lot more on this in the blog “Mark and Jarod Hate Manual Therapy”). I am however, saying that the biomechanical aspects of manual therapy you were most likely taught and educate your patients on are inaccurate at best and harmful at worst. You could possibly be creating a nocebo effect by portraying the idea of a weak and fragile body that cannot easily withstand the forces of daily life without “getting out of whack”. Taking a step back to consider what manual therapy can and can’t do is valuable not only for your own critical thinking/clinical reasoning, but also for the patients you interact with every day.
Want to learn how to best use manual therapy in the clinic?
Dr Mark Bishop has done a Masterclass lecture series for us on:
“Manual therapy in the 21st century”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Leave a comment (1)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
how to publish a research article…? can you help me