
I have had the opportunity and privilege to work with overhead athletes in general and handball players in particular for the past 18 years. The overhead athlete’s shoulder, and especially the thrower’s shoulder are very complex, with a lot of challenges in diagnosis and management, not least return to maximum throwing. In this article I will try to give brief overview of how I work with these athletes with a focus on the return to sport (RTS) phase.
The burden of shoulder problems in overhead athletes
Shoulder problems are substantial in overhead sports, such as baseball, softball, handball, volleyball, cricket and tennis (1-11). The overuse injuries are dominant in most overhead sports and are often persistent, with recurrent flare-ups with a risk of players becoming “chronic rehabbers”.
How many return to overhead sports after shoulder injury?
The RTS rate in overhead athletes in the literature is scarce and so is the time to RTS. Most of the studies that have evaluated the RTS rates in overhead athletes are performed on specific diagnosis like Superior labral anterior to posterior (SLAP) tear or glen-humeral instability, and baseball is by far the most common sport that has been evaluated. Depending on type of injury, level and sport, 20-94% of the athletes have been reported to RTS (12-15). This highlights the fact that many throwers with major shoulder injuries don’t return to the their pre-injury level.
Depending on the type of injury and if the treatment is conservative or not, the initial phases of the rehabilitation may differ. For instance, the initial rehabilitation phase of SLAP-injury or biceps tendon pathology may look different compared to rotator cuff pathology, same thing with an unstable shoulder compared to a stable. However, further down the road the focus will be more on strength and conditioning of the shoulder as well as the kinetic chain and throwing.
What is the worst thing you are going to expose your shoulder to on a regular basis? That is in the end what you need to be prepared for!
Depending on the type of overhead sport, the athletes will have slightly different demands on the shoulder. In non-contact sports such as tennis and volleyball, contact injuries are less common compared to handball and water polo where in addition to throwing there are also a lot of clinching with opponents and blocking shots. But in general these are the rehabilitation phases leading the athlete back to throwing striking;
1. Restoring full and pain free range of motion and strength
Ideally, you have pre-injury values of the athlete’s ROM and strength as a reference. If this is not the case, the uninjured shoulder can be used as a rough reference, however, side-to-side differences in ROM and strength in overhead athletes have consistently been reported in the literature. This is something to consider when using the uninjured shoulder as a reference.
During this phase focus should be not only on shoulder strength but also on strength and conditioning of the whole system e.g. lower limb, pelvic and trunk.
2. Introduce plyometrics and power strength exercises
When adequate strength and ROM have been reached, plyometric and power exercises are introduced. The strengthening phase serves as a building block for plyometrics and the plyometrics serves as a transition into throwing.
3. Introducing the throwing programme
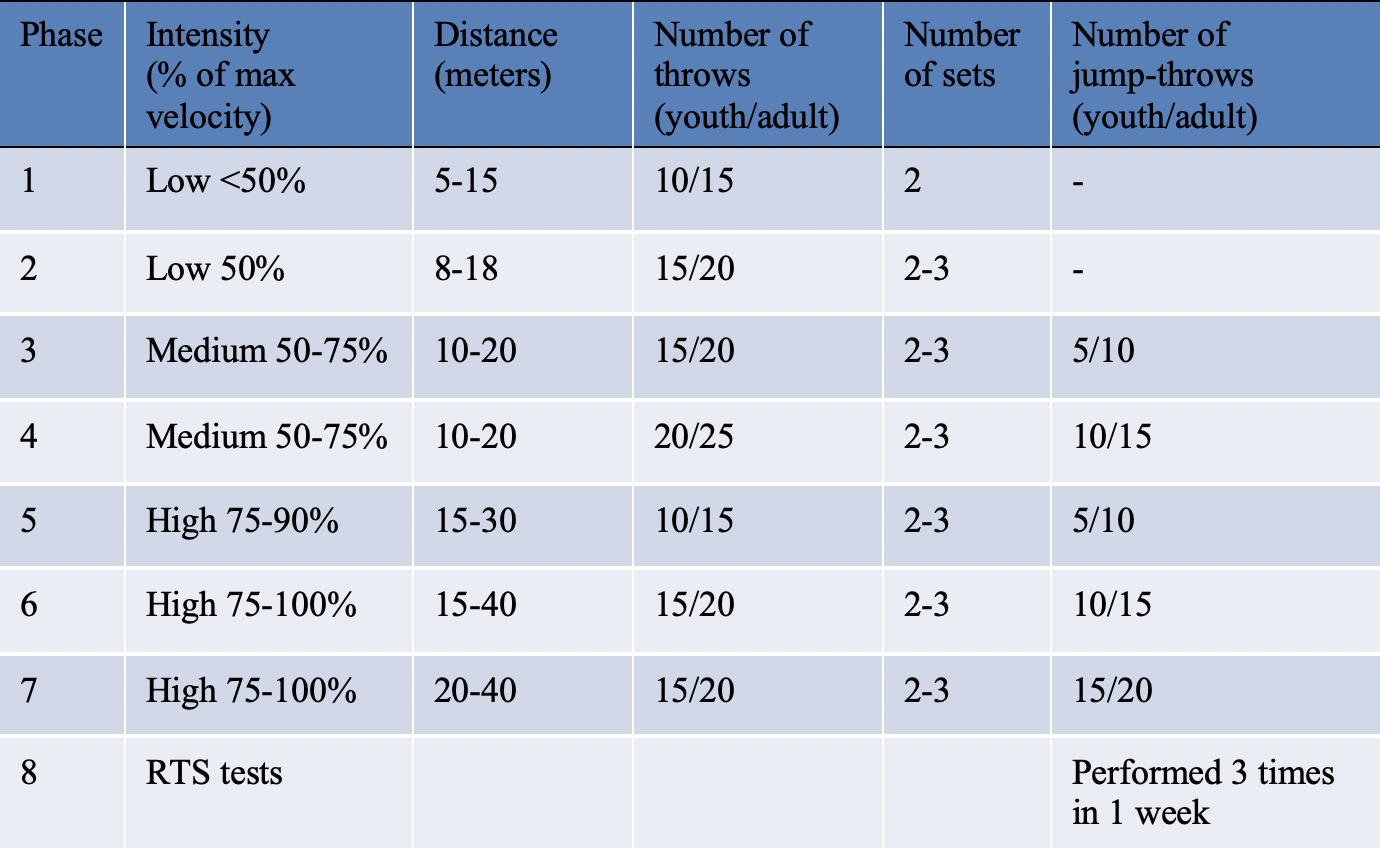
At the end, there is nothing that will prepare the athlete for throwing better than throwing. But we have to get there stepwise. Below is an example of a throwing programme for handball players that I often use as a base, but there are several recommended programmes in the literature, mostly for baseball pitchers (15, 16). The criteria I use for entering the throwing programme is; no reproduction of the athlete’s pain during 1) “break test” (in each direction with a HHD), 2) the previous exercises and 3) pain free full ROM. The programme should be performed every other day to allow one day of recovery and evaluation. No pain is allowed during the programme and the programme is designed for 2-4 sessions on each step without any symptoms. If any pain occurs, the athlete has to drop down one step. If the athlete isn’t a thrower this phase can be modified to match the demand e.g. tennis serves or volleyball spikes instead of throws.
4. Evaluate strength, ROM and workload
Through the throwing programme the athlete has to continue the strength and conditioning programme. To ensure that adequate progress is made, strength, ROM and workload should be measured objectively throughout the rehabilitation, preferably with a hand-held dynamometer and an inclinometer and session RPE.
5. Perform return to play tests and make shared return to play decisions
Spoiler alert! There is today no evidence based RTS test to check if the athlete is ready to return to throwing. There is no test or test battery that will say ‘if you score this on this test the chance of returning to maximum throwing without getting a re-injury is xx %’. So, as practitioners what do we do? Will still have the athlete in front of us, and we still need to make decisions and give recommendation on RTS. Well, again we have to ask ourselves, what is the worst thing the athlete will expose their shoulder to on a regular basis. Not the average demand on the shoulder or the average number of throws, but the worst-case scenarios. If the demand only includes throwing then the throwing programme as it is can serve as a test, but if the sport also includes other elements like clinching, blocking and falling/landing on the shoulder then these elements should be included in the tests as well.
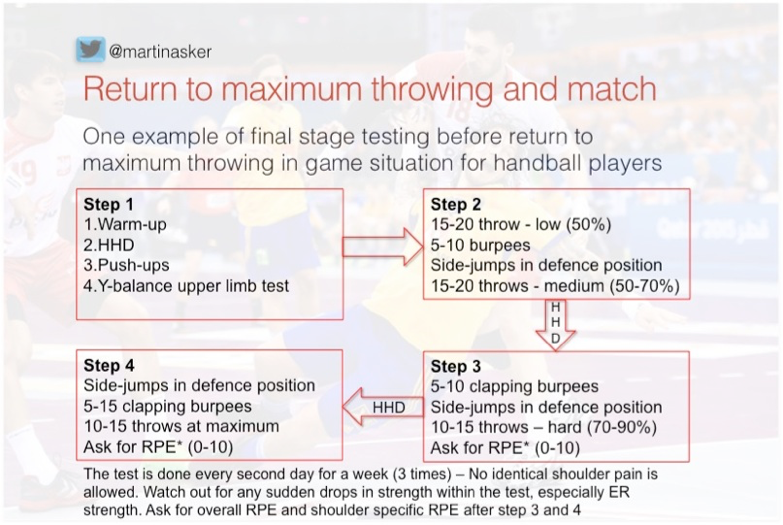
Below is one example of a RTS test that I use as a base for handball players. The test includes several steps where strength, RPE and shoulder symptoms are evaluated between each step. The test is designed to simulate the elements of handball. The test is performed 3 times with one days rest and if the test reproduces their pain the test ends and we go back to the ‘drawing board’. Other than pain I look for any rapid drops in strength. In my experience, the players drops around 10-15% in ER strength and increase 10-20% in IR strength during the test. If a player drops more than that, then that’s a heads up for me that the player probably isn’t ready yet. The player should then continue with the strength and conditioning and the throwing programme with a new evaluation made later on.
More than just strength and conditioning
Now, physical fitness is not all that matters. The player has to be confident returning to the sport. There are several questionnaires to use to evaluate this but I keep it simple, especially with the younger athletes and just ask them to grade their confidence from not confident to super confident and super confident is what I’m looking for. Often as a clinician you build a relationship with the athlete and sometimes you are the only person that the athlete will honestly share such information with.
Finally, the RTS decision should be a shared decision based on the diagnosis and symptoms, the tests described above, together with an assessment of the overall risk of returning to sport. This decision is made together with all the stakeholders e.g. the medical team/clinician, athlete, coach and parents. This is described very nicely and discussed in the 2016 consensus statement on RTS (17).
6. Return to performance
Return to sport/throwing is not the same as return to high performance. Returning to high performance phase should be seen as a continuum that overlaps the return to sport/throwing phase i.e. the performance enhancement will continue after the athlete has fully returned to sport since in many sports, it is during the competition they will gain those last percentage in performance.
In summary
The evidence for RTS rates, time to RTS and RTS tests/criteria in overhead athletes is limited
Criteria should be based on sport specific demands and known risk factors
Also consider athlete specific criteria (playing position, level etc.)
Use sport specific RTS tests and assess for the worst-case scenarios
Always try to avoid spiking the workload but especially post RTS
RTS should based on shared decision with all stakeholders
Want to learn more about shoulder injuries?
Rod Whiteley has done a Masterclass lecture series for us on:
“The sporting shoulder”
You can watch it now with our 7-day free trial!

References
Don’t forget to share this blog!
Leave a comment (2)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Hi Fran!
Thanks for pointing this out.
We have updated the blog now and changed the position of youth and adult.
Hi Martin – thanks for the post. I have a question regarding the number of throws stated for adult and youth in the throwing programme table. What is the reasoning behind those numbers and the fact that youth numbers are higher?
Thanks,
Fran