Assessment of Acromioclavicular Joint Injuries

Introduction to ACJ Injuries
The acromioclavicular joint (ACJ) is a diarthrodial joint comprising the distal, flattened end of the clavicle and the medial aspect of the acromion process of the scapula. ACJ injuries account for 10% of all shoulder injuries that seek medical attention, and 40-50% of shoulder injuries in the athletic population (1). ACJ injuries are 5 times more common in men, and are common in overhead sports but more often involve collision sports such as rugby. Despite being so common there is no consensus regarding optimal management of ACJ injuries (2). Before we delve into ACJ assessment, let’s briefly review our anatomy.
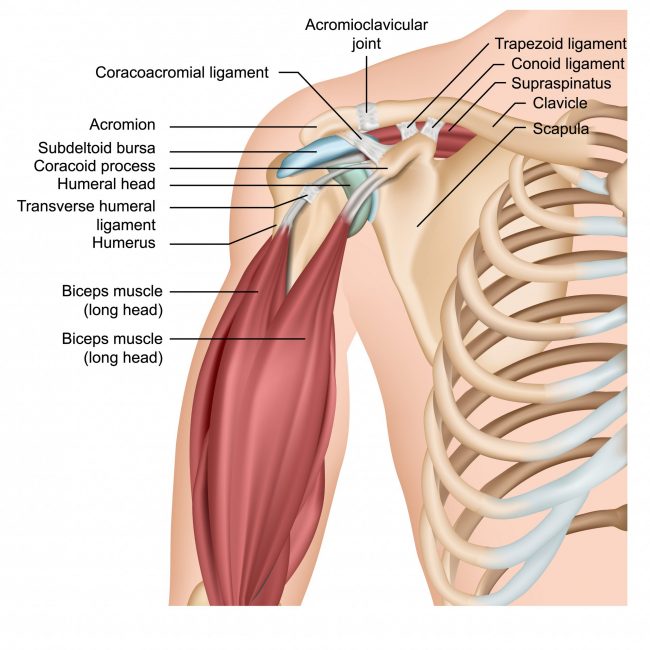
Relevant Anatomy
The ACJ consists of static stabilisers and dynamic stabilisers which include the deltoid and trapezius muscles. Static stabilisers include the AC capsule, the acromioclavicular (AC) ligaments and the coracoclavicular (CC) ligaments (including the conoid and trapezoid ligaments). The AC and CC ligaments resist posterior translation of the clavicle and axial rotation (3). Understanding this anatomy is vital when you assess someone who you suspect has an acute ACJ injury.
Mechanism of Injury
The mechanism of injury is most often a direct fall on the outer aspect of shoulder with the arm in adduction, which displaces the acromion inferiorly and medially. The AC ligaments are the first to fail, allowing the load to be transmitted to the CC ligaments. Disruption of CC ligament leaves the trapezoid and deltoid muscles to act as restraints. Higher forces can lead to rupture of these muscle attachments as well (2). All these structures are assessed as one united role when grading the injury using the Rockwood Classification.
The Rockwood Classification
The Rockwood classification is the most widely used system for ACJ injuries, with grading based on radiologic measurements (4). It categorises ACJ injuries into 6 grades and describes a sequential pattern beginning with AC ligament disruption, CC ligament disruption and subsequent delto-trapezial fascial disruption.
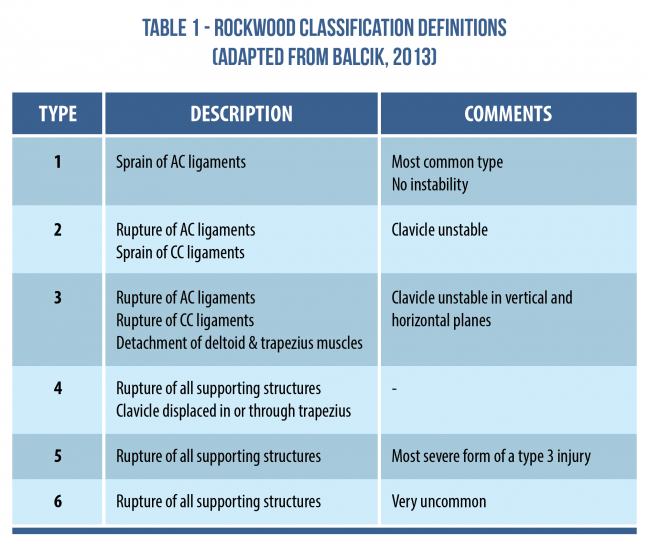
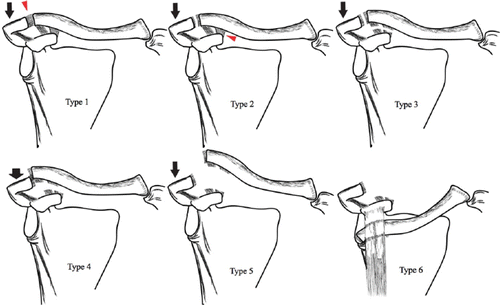
Characteristics of Rockwood Classification (5)
However, the limitation of the Rockwood classification is that it is a diagnosis made from imaging and does not consider the patient’s clinical symptoms or functional demands. Some studies suggest that there is no correlation between the Rockwood classification and the degree of pain and function (4, 6). This is vital as imaging is often used to dictate early surgery or a conversative first approach.
There is also a lack of agreement amongst surgeons regarding the classification of type 3 and 5 injuries which contributes to the substantial variation in the classification, diagnosis, and management of ACJ dislocations. “An ideal classification system should be reliable, reproducible, clinically useful, an accurate guide to treatment and should be able to predict prognosis which the Rockwood does not provide” (6).
Instead of relying on the Rockwood classification, a thorough subjective and physical exam including the use of imaging is essential to guide your decision making.
Objective Assessment
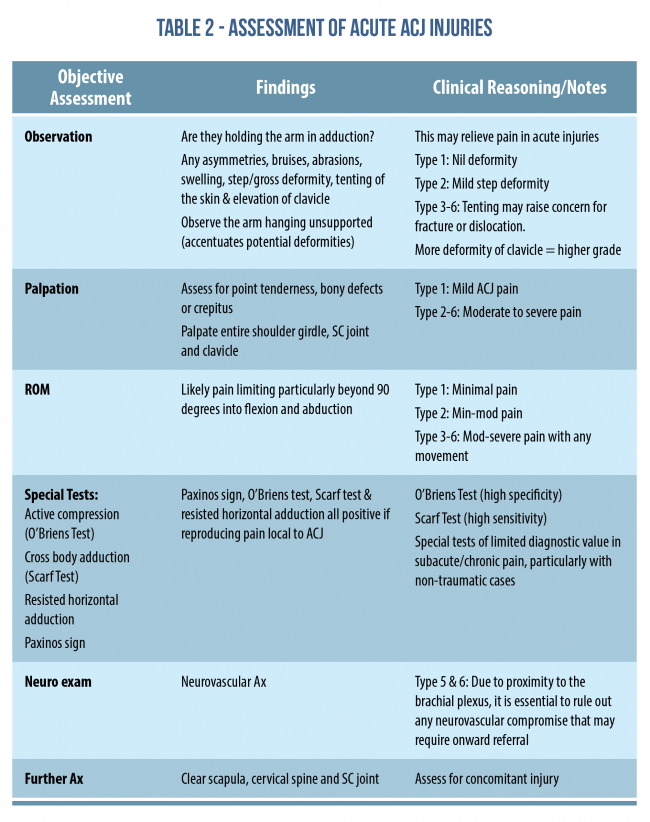
After you’ve ‘’received’’ (hat tip to David Poulter) the patient’s history, you’ve listened to them and understand their story, it is then time to conduct your physical assessment. As part of this exam, imaging can be used in conjunction with your assessment as certain examination findings may be linked with the Rockwood classification. This becomes more important when differentiating between type 3 and type 5 injuries and the management they require. Some authors suggest that these injuries can be distinguished based on the integrity of the deltotrapezial fascia which are evaluated by actively shrugging the shoulders. This motion may reduce type 3 injuries, but not type 5 (3).
Below is a table of common ACJ assessments along with potential findings (7).
For more information on conducting the clinical exam for ACJ pathology, see Rod Whiteley’s Masterclass on The Sporting Shoulder.
ACJ Injuries – Is it all about trauma?
Although this blog is focused on acute ACJ pathology, it is worth mentioning that not all ACJ injuries come after trauma (1). The ACJ can also be a source of osteoarthritis and rheumatoid arthritis, with symptoms referring to the deltoid and neck. In advanced rotator cuff pathology, joint cysts are possible where there is a palpable lump over the ACJ (commonly referred to as a Geysers Sign on imaging).
A combination of atraumatic and traumatic ACJ pathology is Distal Clavicular Osteolysis (DCO). Clinical presentation of DCO includes pain, point tenderness, soft tissue swelling and reduced function, and is diagnosed with both clinical and radiological findings. Atraumatic cases are associated with chronic repetitive stress related to weightlifting and overhead sports. MRI is the most sensitive for early detection of DCO and may include characteristics such as bone marrow oedema or periostitis (1).
Conclusion
This blog briefly outlined the anatomy, mechanism of injury, issues surrounding the radiological classification of ACJ pathology, and how to assess acute ACJ injuries. In part 2, we will explore management of various ACJ pathologies with the aim of helping you to optimise care for your patients. If you’re overwhelmed with excitement and can’t wait for part 2, then be sure to check out Rod Whiteley’s Masterclass which covers ACJ injuries in depth.
Want to learn more about shoulder injuries?
Rod Whiteley has done a Masterclass lecture series for us on:
“The sporting shoulder”
You can watch it now with our 7-day free trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!