
Fracture of the base of the fifth metatarsal is one of the most common stress fractures encountered in the lower extremities (1). According to recent epidemiological studies, this fracture accounts for almost 40–75% of all fractures encountered at the foot (2). Moreover, studies report that the onset of this fracture at the fifth metatarsal’s base is highly prevalent in both sports and sedentary settings (3, 4). For more on stress fractures, I highly recommend checking out Dr Stuart Warden’s Masterclass on Bone Stress Injuries here.
The biomechanical insufficiency of the fifth metatarsal during inverse axial-loading at the ankle joint has been suggested to be a predominant reason predisposing towards this stress fracture. Secondly, a higher correlation between metatarsal fractures and lower levels of bone mineral density as in osteoporotic, and post-menopausal women, is an additional reason why fracture is common in older population groups (5). Typically, the management of base of fifth metatarsal fractures has been pursued by either operative or non-operative measures (6, 7).
Nowadays, the term ‘Jones fracture’ defines just one type of the fifth metatarsal fracture, that is a ‘Zone 2’ injury, and there are several misconceptions and controversies regarding the terminology and treatment of these injuries.
Appetizer
Over the years, numerous classification systems have been created. The most widely used
classification is that of Lawrence and Botte (1993).
- Zone 1: Tuberosity avulsion fractures with or without involvement of the tarsometatarsal articulation (’pseudojones‘ or ‘tennis’ fractures) – most common, accounting for more than 90% of the fifth metatarsal fractures.
- Zone 2: Fractures of the metaphyseal–/diaphyseal junction, which extend into the fourth–fifth intermetatarsal facet, distal to the articulation between cuboid and fifth metatarsal base (‘Jones’ fractures).
- Zone 3: Proximal diaphyseal stress fractures, typically located distal to the Lisfranc joint and distal to the fourth–fifth intermetatarsal facet, that is in the proximal 1.5 cm of the metatarsal shaft.
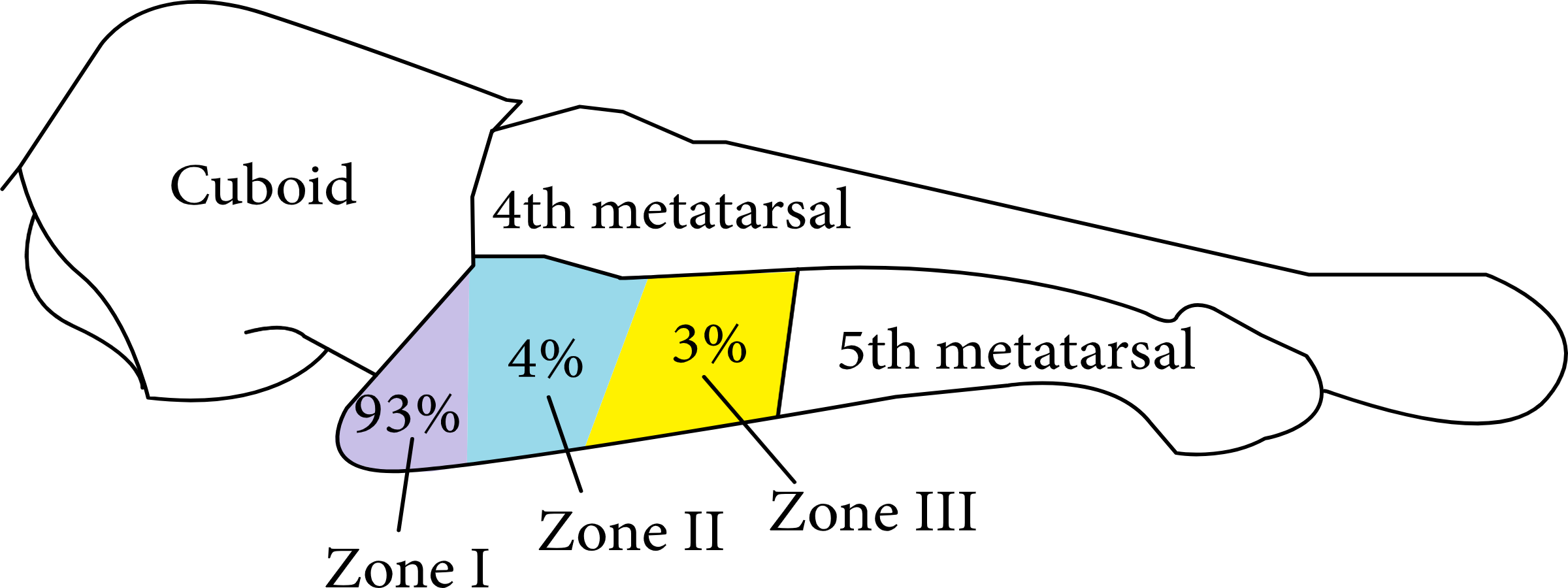
Figure 1 (8)
Mains
Despite advancements in the past decade concerning development of various interventions and anatomical specifications, a consensus surrounding an optimal choice of intervention for managing base of fifth metatarsal fractures is still lacking. On one hand, part of the literature recommends the aggressive use of operative intervention because of their ability to enhance the rate of fracture union, duration of union, and duration of return to sports.
Conversely, other literature recommends the use of non-operative interventions to facilitate recovery. The studies suggest that the use of non-operative interventions can avoid the complications, discomfort associated with the surgery and that too in a cost-effective manner (6, 7). In addition to that, recent systematic reviews provide inconclusive evidence regarding the optimal choice of treatment (9, 10). Taken together, this lack of consensus has proven to be a challenging avenue for the clinicians to develop an efficient decision-making model for selecting optimal interventions for managing the base of fifth metatarsal fractures.
The patient’s history and physical examination is paramount to differentiate between an acute or stress fracture. Patients with acute fifth metatarsal fractures present with pain, localized swelling and tenderness, difficulty in walking or weight-bearing, and in some cases, bruising.
Patients presenting with stress reactions or fractures complain about pain only during activity in certain phases of the GAIT cycle (toe off), with these symptoms commonly being present for several weeks. Generally, patients are able to localize the pain to the area of the fracture, while foot inversion from 30 to 50° results in maximal strain and increased symptoms.

Predisposing factors for stress fractures such as previous history of a stress fracture, recent intense (or change in) activity, osteopenia, and endocrinopathies (diabetes mellitus, hyperparathyroidism, nutrient deficiencies etc) should be identified. Serum calcium, vitamin D, nutritional deficiencies, and history of menstrual cycle irregularity in females should be evaluated, as these can unveil metabolic bone pathologies. Finally, a comprehensive foot and ankle examination is of utmost importance, with the entire lower limb being evaluated.
Dessert
Nondisplaced zone 1 injuries can be treated conservatively with protected weight-bearing in a hard-soled shoe, walking boot, or walking cast. Progression to weight-bearing as tolerated can initiate as pain and discomfort subside over 3 to 6 weeks.
Nondisplaced zone 2 injuries, or Jones fractures, may also be treated conservatively with 6 to 8 weeks of non-weight bearing in a short leg cast/boot. The physician may advance weight-bearing status as radiographic evidence of bone healing appears. Indications for surgical interventions include the high-performance athlete, the well informed patient who elects to proceed with surgical treatment, or displaced fractures.
Diaphyseal zone 3 stress fractures paint a more complicated picture for the patient and physician. A trial of conservative management with non-weight bearing in a short leg cast/boot may be the initial therapy; however, immobilization for up to 20 weeks may be necessary before there is observable radiographic union, and even then, non-union development is not uncommon.

Conservative vs surgical treatment is decided based on the fracture type, associated injuries, and individual patient characteristics. Controversies remain regarding surgical treatment options for fifth metatarsal fractures. Nevertheless, depending on the zone of fracture, several of these may be treated non-operatively; however operative fixation with intramedullary screw and possible biologic augmentation especially for the elite athletes with Zone 2 and 3 injuries remains the standard of care.
In contrast, patients who are deemed ‘high risk’ for surgery with a predisposition to complications, for example vasculopathy or patients with diabetic neuropathy, should be treated non-operatively. Moreover, research demonstrates significantly enhanced treatment outcomes as assessed with American orthopaedic foot & ankle scale score (AOFAS) for the operative interventions as compared to non-operative interventions.
Wrapping up
This was a whistle stop tour outlining the evidence for the management of 5th metatarsal fractures. For more on stress fractures, I highly recommend checking out Dr Stuart Warden’s Masterclass on Bone Stress Injuries here.
Want to become an expert on plantar fasciitis?
Dr Henrik Riel has done a Masterclass lecture series for us!
“Diagnosing and managing plantar heel pain”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!