The ACL Healing Phenomenon: Science or Myth?

Up until around 8 years ago, I was ambivalent towards ACL tear injury management, and even as a Masters-trained Senior Physiotherapist if pressed, probably assumed reconstruction was ‘gold standard’, as that’s what I’d read and seen everywhere.
It was 2 opposing cases I saw in quick succession as a trainee Specialist Physiotherapist that confronted me head on, forcing me to challenge any bias I had and avail myself to the best research literature (1).
1 of the patients had experienced 5 ACL surgeries, presenting to my clinic on a 4-wheeled-walker (which was incredibly odd for a woman in her mid-30’s). She was stressed, depressed, anxious, suicidal and had clearly not received adequate supervised post-op education and rehabilitation over the 4 years her operations had taken place.

The second patient had a fresh ACL and meniscus injury, who was adamant on commencing rehabilitation without surgery, as her sports teammates had experienced failed elective knee surgeries. We crafted a management plan in a shared decision-making context, began rehab and she returned to play at 4 months and at long-term follow-up remained sign and symptom free.
This forced me to question the orthodoxy that is ACL recon as ‘best practice’, spending 100’s of hours investigating the most credible evidence, with help from both Surgeon and Physiotherapist researchers and expert clinicians. What I discovered was that Westernised culture was flooded with a one-sided narrative of ACL reconstruction as the best first choice based on old bio-plausible, pathoanatomical paradigms, with this Global multibillion-dollar per annum gold-rush perpetually funded by governments, private insurance companies and commission-style private hospital sectors, with the best-evidence and patients falling second place (2).
Since that time, the ACL topic has absolutely mushroomed for me, whereby now I have overseen 1000’s of full thickness tears managed without surgery, including patients who have returned to high-level pivoting, jumping and cutting tasks.
Want to learn more about non-surgical management of ACL tears? Check out Kieran’s fantastic Masterclass on this topic HERE.
Can ACL ruptures heal?
In the past 3 years, my management approach has shifted, due to a growing awareness of the healing capacity of ACL tears. I regularly see full thickness ruptures heal, with confirmation on repeat-MRI. This is a significant turn in clinical reasoning and management for me. A cursory Google search will reveal most initial websites suggesting “ACL tears never heal”, they have a “poor blood supply” and “surgery is necessary” to return to sports.
Fresh investigations have exposed online surgical advertising content by private elective orthopaedic groups targeted towards patients is frequently false or misleading (3, 4), over-estimating the benefits of surgery and under-estimating the harms (5), with calls for government regulators to intervene. We must wonder where the obsession with reconstruction experimentation will end, with kangaroo tendons and gold nanoparticles touted as the next big thing (6, 7).
A systematic review showed that ACL full thickness ruptures CAN heal, with strategies including bracing, rehabilitation and strengthening and even no management at all (8, 9).Shifting the burden of proof, the authors highlighted the revelation there are in fact no high-quality studies showing the ligament CAN’T heal! In a national debate on ACL tear management which I was a part of at the end of 2021, Physiotherapists, Surgeon researchers and expert clinicians agreed ACL tears can heal. Pilot data from Australia due to be released in 2022 was discussed, with over 90% of fully ruptured ACL’s healing with a novel bracing protocol, and long-term return-to-play achieved.
The ground-breaking KANON study revealed 58% of those who did not cross over to surgery had MRI proof of healing at 5-year follow-up (10). High healing rates have also been proven in partial tears with the use of a bracing protocol (11). Normalised anatomical, partial, lengthened ACL and non-anatomical (such as proximal ACL bundles attaching to the PCL) are all possible types of healing (12, 13, 14). Orthopaedic surgeon Andrea Ferretti stated that the ACL’s “blood supply.. is rich in vessels and anastomosis, providing adequate supply to all kinds and sites of tears,” with others recently suggesting increased blood supply following an ACL injury (15, 16).
Shared decision making
Shared-decision making is key here (17), meaning patients must be told their ACL tear may or may not heal as a part of their management options, although I do worry that in the ‘real world’ it is a pipe dream given our post-evidence-based era (18, 19). A Telehealth client of mine in 2021 saw a medical specialist who informed her that “a bomb had gone off in her knee,” her “knee had exploded” and her “only option and solution was surgery:” She had a partial ACL tear – talk about nocebo.
Not surprisingly, she burst into tears and under fear-mongered duress booked in for a reconstruction the following week. By chance, she was able to connect with me, we commenced a stabilisation protocol, with a follow-up MRI displaying near intact healing of the ligament; she returned to semi- professional soccer without surgery and at long-term follow-up is incredibly satisfied with her decision to wait and consider her options.

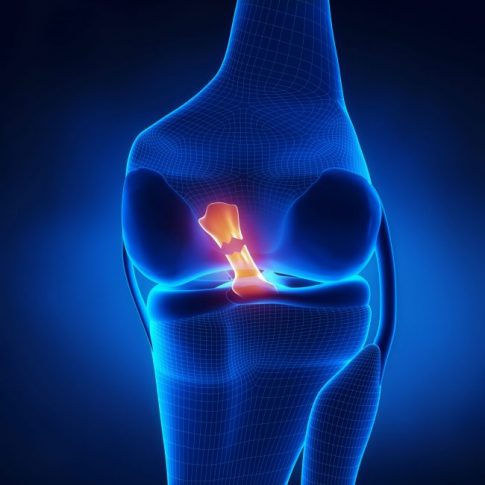
Figure 1: 28-year-old ACL-injured patient with an MRI at 1 week, and long-term follow-up (Park et al 2021)
In my experience, almost all patients aren’t given an objective shared decision-making process. This takes time (more than a 15-minute consult), care, empathy and empowerment of patients with current best guidelines, education aids, infographics and resources (20, 4). Communication has to be calm, unbiased and honest, with potential risks, harms and benefits of all treatment options clearly unpacked. A level-2 long-term cohort study showed incredibly high knee reinjury rates, with 2 out of 3 reconstructed patients suffering further damage after return-to-sport (2); these types of patients are often led to believe surgery is a “one-way ticket” to return to sport (22).
Studies of poor methodological quality, which retrospectively compare ACL reconstruction and rehab to non-controlled or absent comparison arms, and mechanistic-theory like ‘a graft-ACL acts like a normal ACL’ cannot be used to justify early reconstruction (23). A common purported misconception is that ACL reconstruction prevents greater rates of meniscal tears to non- surgical management (24). However, this evidence is considered as too weak to guide surgical treatment decisions (25). Both KANON and now the COMPARE randomised control trial have shown similar meniscal tear rates over time, with COMPARE actually showing higher future meniscal surgery in reconstructed patients (26, 27).
Who should have surgery?
We need to be advising all patients that the most empirical evidence shows no additional benefit of ACL reconstruction, meniscectomy or meniscal repair to rehabilitation alone for knee-injured patients, with no high-quality studies proving superiority of these techniques over exercise therapy treatment or placebo surgery (28). A Professor of Orthopaedic Surgery I met commented that he tells ACL and meniscus-injured patients “to go away and complete 6 to 12 months of rehabilitation on their knee” and he will then “operate on their knee if they aren’t satisfied” because he “can’t promise their knee will be better long-term for being operated on early.”
None of this is to say reconstruction is not a viable option for patients who have recurrent episodes of hard instability, despite an early administered high-quality stabilisation protocol; I have reiterated this in mass media interviews and have collegial connections with pragmatic orthopaedic surgeons who I collaborate with and share more in common with in managing musculoskeletal pain and injury, than not.

Physiotherapy leading ACL management
I believe Physiotherapists can be the leaders of managing ACL injuries in a triage role, which has been successfully implemented in musculoskeletal pain and injury primary care policy shifts in countries like Denmark and the UK, which can have a multiplicity of benefits to governments, private insurers, the medical system, patients, and clinicians alike (29).
Kiadaliri et al (2016) suggest savings of over $20,000 (AUD) in costs per patient through a fiduciary shift towards a Physiotherapy-led approach, reduce resource consumption and decrease risk of unnecessary overtreatment, even with the option of reconstruction, if needed (30). Interprofessionally, we need to all work together to design large, multicentre trials to assess healing capacity of ACL tears in various demographics, so patients can hopefully be triaged early, and significant amounts of money saved. If only this had been done 60 years ago, when the theory that ACL tears can’t heal was propagated based on animal models!
Wrapping Up
We as a profession will never be anti-surgery, but also need to represent patients as strong and confident expert non-surgical advocates by describing the best comparative evidence treating ACL and meniscus tears with exercise alone, weighed against surgery and exercise. If we won’t, who will?
Want to learn more from Kieran? Check out his Masterclass on ‘Non-surgical Management of ACL Tears’ HERE.
Want to become more confident treating ACL tears non-surgically?
Dr Kieran Richardson has done a Masterclass lecture series for us on:
“Non-surgical Management of ACL Tears”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Leave a comment (4)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
I had a Grade 3 ACL 2 weeks ago, 31 December 2022. I am really scared to go for a surgery, Is conservative will work for me? I would rather opt for a life time commitment exercise rather than having surgery. Please advise.
the future will be interesting indeed. for now, i do think that simple acl tears (without concurrent meniscal and MCL injuries) would have a better chance of healing and .: respond better to rehab. would be great to find out what populations do heal and to eventually have a protocol for it (i.e. bracing and some triage for who should go to surgery – likely failed conservative management cases). I guess the elite athletes often do not have the time to see if conservative management will work before doing a surgery as they are often a limited time schedule.
Great blog! Thank you. My ACL took about 1 year, but my first 4 months were focused on rehabilitation of 12 spinal fractures, so it may have been a little sooner if specific rehab was started earlier.
Awesome!!
This is great information!!
But you missed our scientific evidence!
Be sure to check it out!!!
https://journals.sagepub.com/doi/full/10.1177/0363546516654687