
Radicular pain (such as sciatica) is a common problem that presents to musculoskeletal physiotherapists and general practitioners. In a recent primary care study in the UK including 609 patients, 60% of people presenting with a combination of back and leg pain were diagnosed with sciatica (1). Due to the high prevalence of sciatica and associated pain and functional limitations, it is vital clinicians can identify radicular pain accurately and differentiate it from other pathologies.
Part 1 of this two-part blog series will aim to help you understand what radicular pain is, how it presents, and outline conditions that can masquerade as radicular pain that could be considered in your differential diagnoses. This blog series is based on Tom Jesson’s fantastic Masterclass – Assessing and managing radicular pain. If you want to dive deeper into radicular pain, be sure to check it out!
Alright, let’s start with some definitions, causes and presentations.
Definition and Presentation
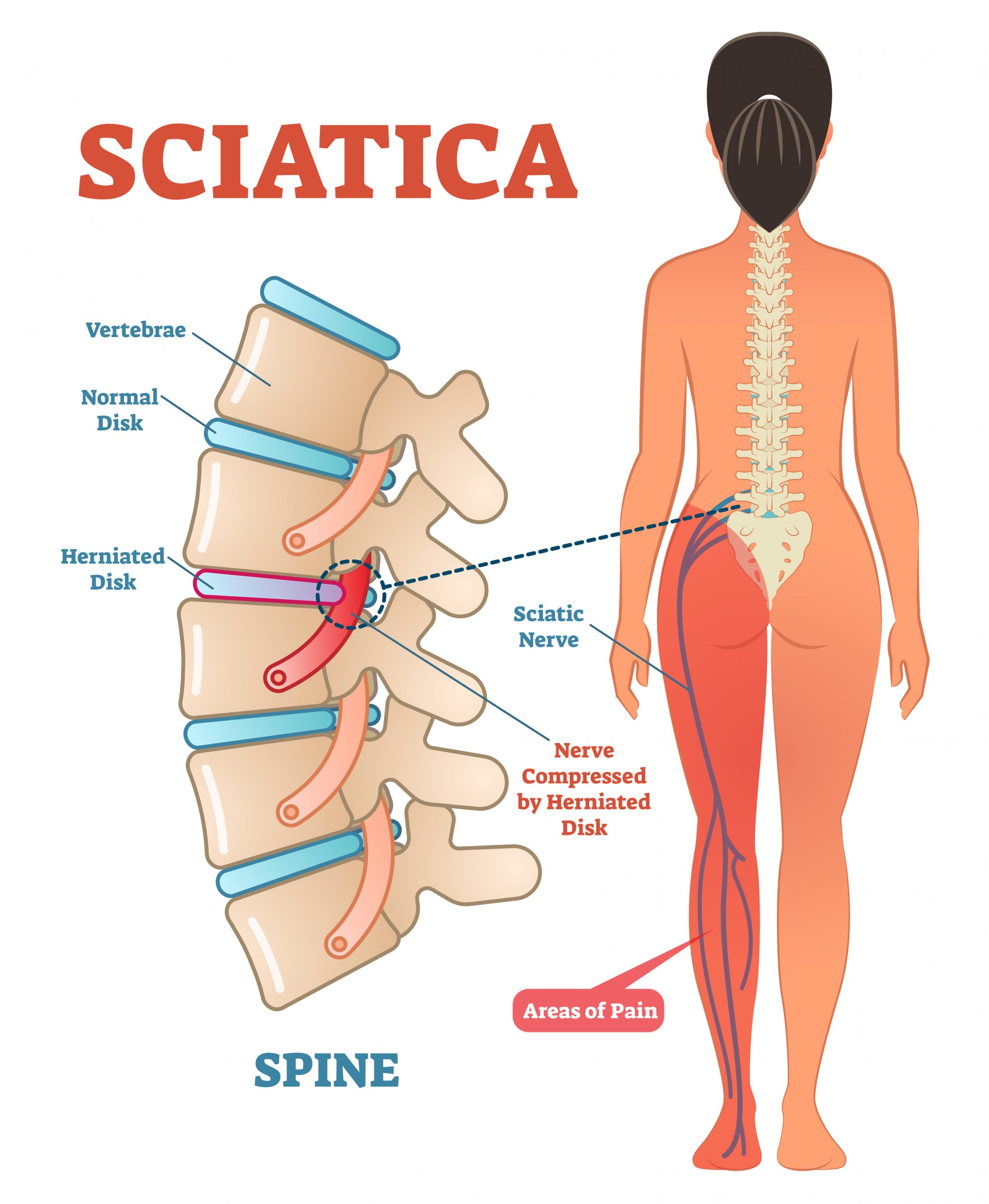
Radicular pain is caused by inflammation and/or compression of the lumbosacral nerve roots (L4-S1) and results in a gain in nerve function (2). This refers to an abnormal excitability of the nerve, presenting with paraesthesia, pain, hyperalgesia, allodynia, hyperreflexia, and/or muscle spasms. Pain often presents in the buttock, travelling down the leg and below the knee.
This differs from lumbar radiculopathy, which is also a nerve root problem, but results in a loss of nerve function. This means there is reduced impulse conduction which may present as hypoesthesia, anaesthesia, weak/absent reflexes, muscle weakness and/or reduced sensation. Unfortunately for practitioners, patients don’t always fit into these categories and it’s therefore not uncommon for patients to present with features of both conditions, such as a painful radiculopathy (3). It’s also important to remember that true radicular pain is an extremely distressing and painful condition, with some patients reporting a loss of their sense of self (4).
In general, sciatica is poorly defined in the research. Whether you are a physiotherapist fresh out of university or have been practicing for many years, you’ll likely have known or heard of someone complain of sciatica. But, how do we know it is definitely sciatica? How do we know the problem isn’t from the sacroiliac joint, the hip or (god forbid) the dreaded piriformis muscle?! Let’s look into some risk factors and causes of radicular pain to help identify the patients that might have a true nerve root pathology.
Risk Factors
To accurately identify someone with radicular pain, it is important to understand the risk factors and causes of the problem. This was very nicely laid out by Tom Jesson in the Physio Network Masterclass on Radicular Pain. If you want a thorough explanation of the history, pathophysiology and management of radicular pain, be sure to check it out. Tom classified risk factors and causes into two groups as documented below.
Distal (The Kindling):
- Smoking
- Obesity
- Manual work
- Work bending down
- Driving a lot
- Moderate walking
- Mental stress
- Poor job satisfaction
Proximal (The Fire):
- Disc lesion
- Spinal/Recess stenosis
- Spondylolisthesis
While this is not an exhaustive list, these are important to consider as part of a comprehensive assessment including your subjective and physical exam.
How is Sciatica Diagnosed?
A diagnosis of sciatica is based on clinical presentation, involving the patient’s subjective symptoms and the findings of the physical examination. There is no specific test for sciatica, but a combination of positive findings on examination increase the likelihood (6). Imaging is rarely required to make a diagnosis unless a more sinister pathology is suspected or if the patient has not responded to conservative management as expected (2). However, if the patient presents to your clinic with imaging already completed, then by all means check to see if your exam aligns with the imaging findings. The key signs and symptoms of sciatica include:
- Dominance of leg pain (more than back pain)
- Location of the leg pain (e.g. below the knee)
- Dermatomal pattern
- Paraesthesia and/or sensory loss aligning with the spinal root
- Myotomal changes
- Reflex changes
- Leg pain when coughing, sneezing, taking deep breath
- Gradual onset
In your physical examination, the below are possible findings:
- Unilateral motor weakness (particularly dorsiflexion if L5 is affected, leading to foot drop)
- Absent tendon reflexes
- Positive SLR (if negative, this reduces suspicion of sciatica)
- Positive cross over test
- Increased finger-floor distance (>25cm)
It is vital that the practitioner can exclude sinister pathology by screening the patient for trauma, cancer or serious infections. If your index of suspicion is low for sinister pathology, it is worth considering if your primary diagnosis of radicular pain is accurate, or if the pain is coming from somewhere other than the nerve root. Other potential conditions that may masquerade as radicular pain are outlined in the below table (7).

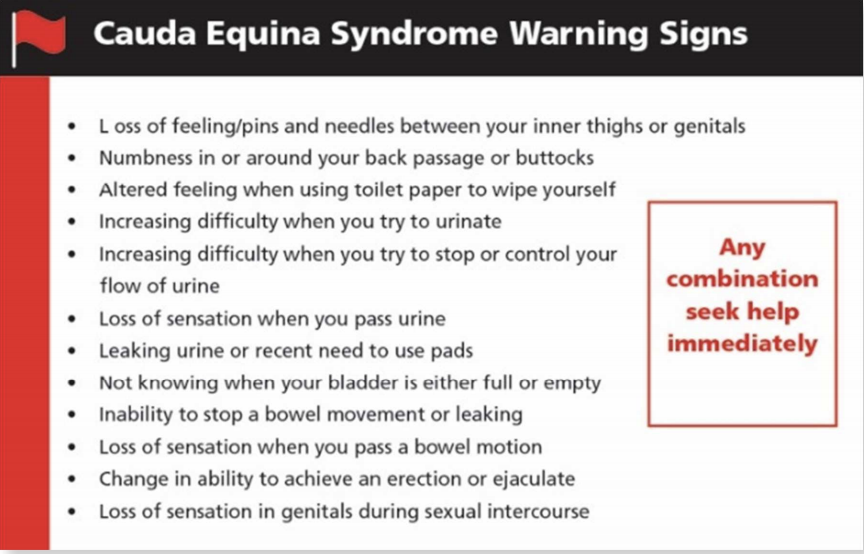
In the case of saddle anaesthesia, disturbances of the bladder, loss of tone in the anal sphincter, decreased sexual function, and/or severe and progressive neurological deficits, a cauda equina syndrome may be present and patients should be referred for immediate medical attention. See the image below for an outline of cauda equina syndrome warning signs (8).
Radicular or Referred Pain?
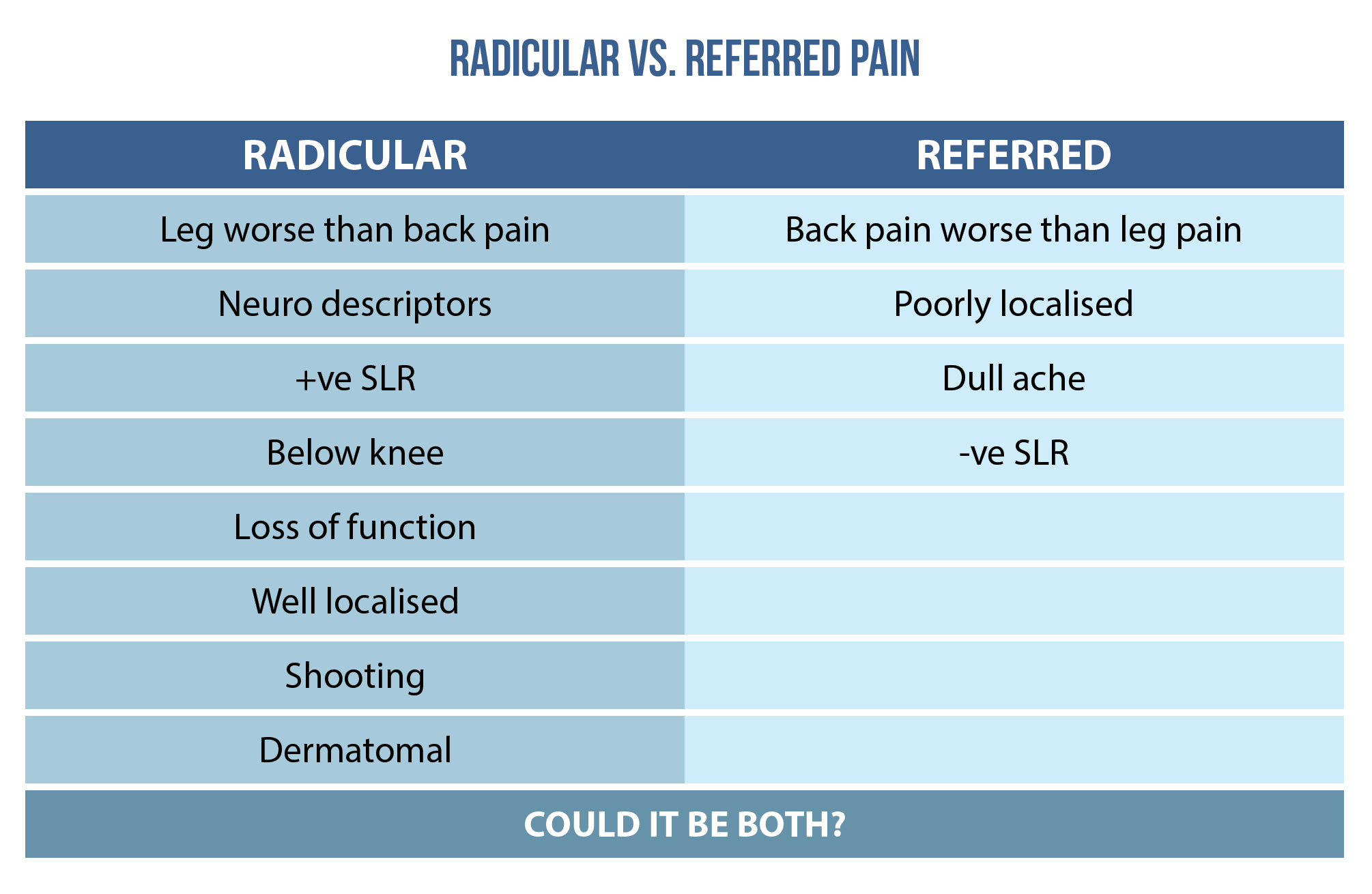
At this stage you may be wondering, ‘’well, my index of suspicion for something sinister is low here, so do I need to know if this is a nerve root problem or not?’’. This is a valid question and for some patients it may not matter. These are the patients who improve without any input from a physiotherapist and naturally recover in expected time frames. However, if a patient isn’t recovering as expected and may require more invasive treatment, it is important our diagnosis is as accurate as possible to provide the patient with the best and most individualized treatment options (stay tuned for part 2). Therefore, it’s worth considering whether this is radicular or referred pain, as Tom outlines in his Masterclass. See the table below for help distinguishing between the two.
Objective Assessment
Your objective assessment should include a neurological exam to investigate the functioning of the nerve. This should involve assessing light touch, reflexes and motor strength. It is worth noting that performing these tests only assesses 30% of the nerve (9). To assess the remaining 70% of the nerve, consider using pinprick or a temperature assessment using hot/cold devices. For more information on this topic, check out Tom’s Masterclass.
Conclusion
To conclude part 1 on the differential diagnosis of radicular pain, you now understand the definition, causes, risk factors, and how to assess someone for radicular pain. We have outlined the importance of considering other pathologies in your differential diagnoses, sinister pathology and conditions that can masquerade as radicular pain. In part 2 we will cover the management of radicular pain so that you can optimize the care for your patients and help them in their recovery.
Want to learn more about radicular pain?
Tom Jesson has done a Masterclass lecture series for us on:
“Assessing and managing radicular pain”
You can watch it now with our 7-day free trial!

References
Don’t forget to share this blog!
Leave a comment (2)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
As a reader seeking clarity on diagnosing radicular pain, I found this blog to be a highly informative and well-structured resource that effectively breaks down the diagnostic process, offering valuable insights and practical guidance for healthcare professionals.
Hello Luke,
Thank you very much for your post! I’m a bit confused when you mentioned the signs and symptoms of sciatica. What do you mean by sciatica here? Is sciatica and radiculopathy one and the same? Or are its symptoms a mix of both radicular pain and radiculopathy?
Thanks.
Jasman PT, Doha, Qatar.