A physio’s guide to Posterior Tibialis Tendon Dysfunction (PTTD)

The tibialis posterior or “tib post” plays a key role in supporting the arch of the foot and facilitating smooth ankle movements during gait. Dysfunction of the tib post tendon can be not only painful, but debilitating – it can impair mobility, and in some cases lead to foot deformities. As physios, understanding the intricacies of Posterior Tibialis Tendon Dysfunction (PTTD) and its treatment options is essential for providing effective, individualised care. In his Masterclass, expert physio Stuart Imer comprehensively covers the anatomy, pathophysiology and typologies of tib post tendon disorders, as well as providing an expert insight into the best-practice assessment and management of PTTD. In this blog, we’ll delve into some of the key takeaways from his top-notch Masterclass, focusing on the most common presentation of tib post tendon issues – midzone pathologies.
If you’d like an in-depth understanding of tib post tendon dysfunction from an expert, watch Stuart Imer’s full Masterclass HERE.
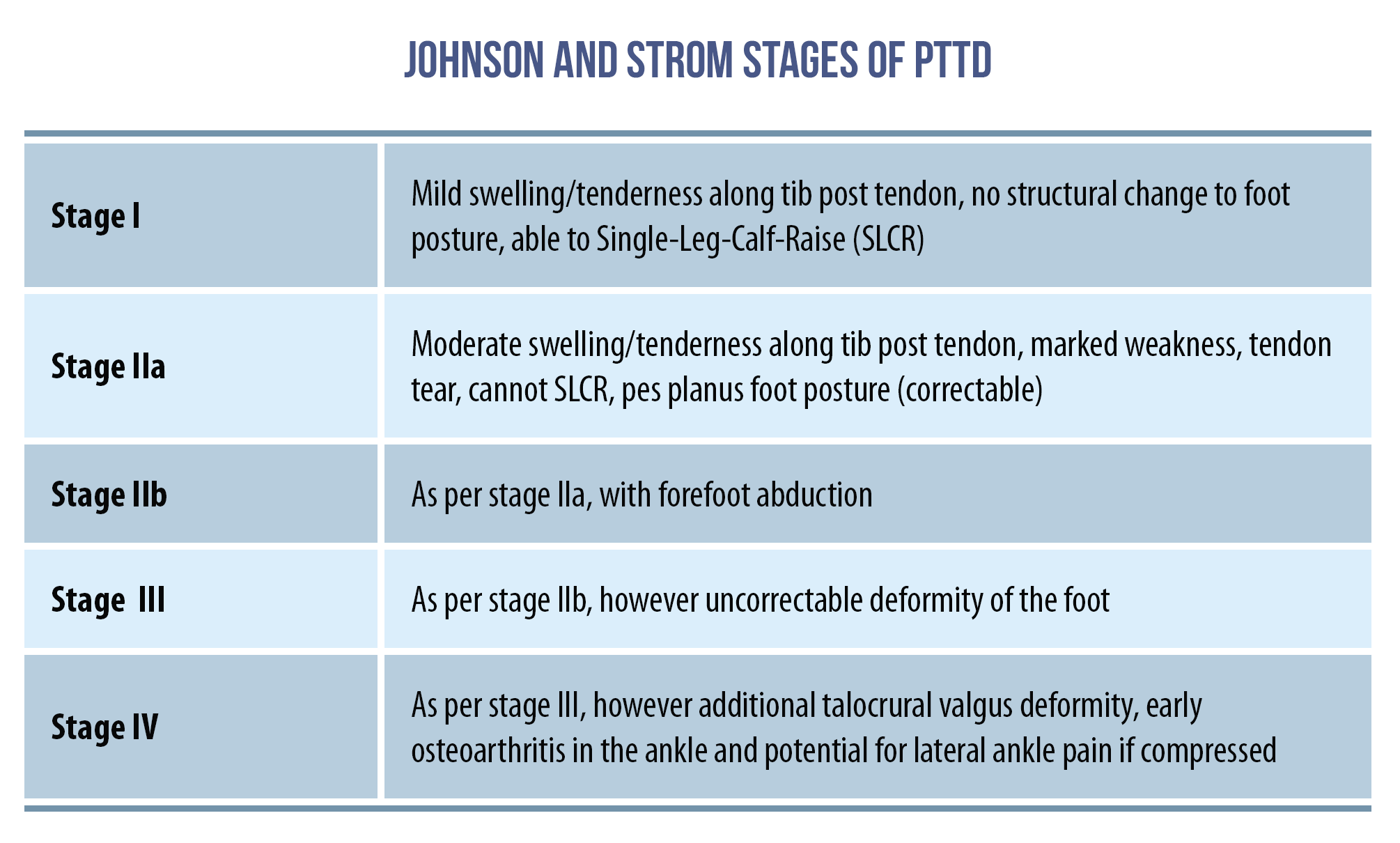
Stages of PTTD
So you’ve identified your patient is experiencing midzone PTTD, what’s next? Midzone PTTD can be categorised under the Johnson and Strom classification system; the below table is a useful tool to use to help guide your management decisions.
Objective assessment of PTTD
Stuart outlines all common objective tests you would expect to complete with suspected PTTD, but now we are looking through the lens of the Johnson and Strom classification system; for example, when looking at foot posture – is there a deformity? Can it be corrected? Stuart notes that he uses a two-foot mini-squat test to assess function and foot posture, watch him demonstrate this in the below snippet taken from his Masterclass:
Obviously it’s also important to palpate the area – this is particularly useful when differentiating between other potential sources of pain, as well as getting a gauge of pain sensitivity and any talocrural joint line pain. Additionally, Stuart notes that gastrocnemius-biased equinus deformity (i.e. reduced dorsiflexion at the ankle due to gastrocnemius tightness) is common in those with PTTD. The Silfverskiold’s test can be a useful way to assess for this – watch Stuart demonstrate this in the below excerpt taken from his Masterclass:
Conservative management of PTTD
Once you’re confident in your diagnosis of PTTD, treatment will include a combination of all your usual suspects – education, load management, ice/anti-inflammatories, taping, orthotics/heel lifts, calf/dorsiflexion mobility and strengthening the tibialis posterior as well as the other structures supporting the medial longitudinal arch. Watch the below video taken from Stuart’s Masterclass in which he demonstrates the taping technique he likes to use with his patients:
It’s important to recognise that the stage of PTTD will likely influence your treatment approach, as the level of dysfunction will dictate your load management decisions and exercise progressions.
Weight bearing
Deloading while remaining active is an important part of tendon treatment; it’s the challenging task of the physio to strike the correct balance between the two. The amount of deloading the patient requires may be determined by the level of dysfunction. Stuart outlines that for a stage I in the Johnson and Strom classification, a short period of unloading with a cam-walker or brace may be useful, but a stage IIa patient could benefit from a short period of partial or non-weight bearing.
Strengthening
As with many tendon issues, it’s useful to start with isometrics. Stuart recommends starting with 10-30 second isometric inversion in a degree of plantarflexion (to avoid over-activation of the tibialis anterior). When appropriate, the patient can progress to weight bearing exercises such as controlled, double-leg calf raises. It’s also important to strengthen the dynamic stabilisers of the medial longitudinal arch including: tibialis anterior, flexor hallucis longus, flexor hallucis brevis, peroneus longus, abductor hallucis, and the calf complex.
For those who are identified to be stage IIb and above, surgical management may be indicated. Generally, there are good clinical outcomes with this population. Stuart outlines surgical approaches and post-op management in his Masterclass, so be sure to watch it HERE!
Wrapping up
Foot and ankle conditions such as PTTD can be debilitating for patients as they can significantly affect mobility and quality of life. Tib post tendon pain requires careful assessment and individualised plans to ensure your patient can get the most out of treatment. Physios play a crucial role in diagnosing and managing PTTD, and are pivotal in helping people regain mobility and function. Stuart Imer’s Masterclass provides a comprehensive description of all things tib post tendon dysfunction.
For a deep dive into the assessment and treatment for tibialis posterior tendon disorders, watch Stuart Imer’s full Masterclass HERE.
Want to get better at treating tib post tendinopathy?
Stuart Imer has done a Masterclass lecture series for us!
“Tibialis Posterior Tendinopathy: Assessment and Treatment Strategies”
You can try Masterclass for FREE now with our 7-day trial!

Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!