How to Make Your Home Exercise Programs More Time Friendly

One of the hardest, yet most critical components of effective rehab, is simply making sure home rehab exercises are done. Some research (1) suggests up to 70% of clients have difficulty with adherence (I hate the term compliance) with a rehab exercise program. There are many reasons for this, many of which I’ve discussed in my article on Failing Physiotherapy (2).
The purpose of this article is to discuss the most commonly addressed barriers of time and to provide you with some great, and uncommon tips to help make your rehab programs more time efficient.
If you are interested in learning more about rehab exercise prescription in general check out many of my other articles as well as the below Masterclasses concerning my two populations of interest:
- Exercise Prescription In Sports Rehab by Dr. Teddy Willsey here
- Exercise Prescription In Aging Adults by Dr. Mariana Wingwood here
First things first – let’s start off on the right foot
I find many of the issues with patient adherence to home exercise programs can be largely mitigated by the following:
- Making sure to clearly explain the reasoning for the exercise(s) and how the exercise(s) benefit the patient goals
- Making sure the treatment is (within reason of course) in-line with expectations
- Asking the client:
- What equipment the client has to exercise with
- How much time the client is 100% sure he/she can put into home rehab exercise everyday
- Hurt vs harm information and educating the client on what an appropriate response to exercise is
There are times where the above may need to be negotiated. Examples include:
- A client who is rehabbing three different body parts probably needs more than one or two exercises.
- Therabands aren’t going to do much for a hamstring strain returning to soccer or a client who has to lift 100 lbs consistently at her job. They need to be pushed harder and may need to look at getting more home exercise equipment and/or a gym membership.

My techniques for time efficiency
Slow eccentrics
Unless you’ve lived under a rock the last five years, you’ve likely seen some posts or research showing the value of slow eccentrics (aka lowering the weight slowly) for improving flexibility (3). It’s so much nicer and easier to give patients a strengthening exercise with a slow eccentric tempo as opposed to doing two separate stretching and strengthening exercises. Slow eccentric tempos also provide an added benefit of creating more stimulus with less weight being required.
Examples of slow eccentrics and their applications include:
- Stiff legged deadlifts: for hamstring flexibility
- Calf raises: for calf flexibility and ankle mobility
- Lunges/Split squats: for hip flexor flexibility (in the rear leg)
- Pulldowns: for shoulder flexion mobility
- Flies: for chest flexibility

Compound movements
Compound exercises are quite popular in the strength training world for the fact that they work multiple muscle groups in the same exercise and are more time efficient. Even though your clients may not tolerate heavy barbell lifts – you can still apply the same concepts to rehab.
Some of the compound movements I like to implement are:
- Pushups (progressing from wall to incline to floor) for chest, shoulder, rotator cuff, tricep/elbow and serratus anterior
- Rows for lats, biceps, rear deltoid and scapular muscles
- Lunges/Split Squats/Stepups/Lateral stepups for quads & glutes
- Carries for grip, shoulders, traps, and core
- Face Pull with external rotation for side/rear delts, rotator cuff, traps and biceps
- B-Stance RDLs or Supported Single-Leg RDLs for back, hamstrings & glutes.
Side note: for both carries, RDL variations & rows, if you don’t have dumbbells or kettlebells you can use a backpack.
RPE
Rating of Perceived Exertion (RPE) is a popular method of reporting how hard you think you are working. It first started for cardiovascular exercise and has been used more recently in the strength and hypertrophy training realms.
I prefer the 0-10 RPE scale where 10 represents Maximum Effort over the 6-20 RPE scale which can be confusing for clients. For people with musculoskeletal pain, I usually instruct clients to perform enough repetitions on each set to bring the difficulty up to between 6-8 on the 0-10 RPE scale.
I almost always use this for clients who are further down the line in recovery, good with exercise form, and just need some high level strengthening. It can also be helpful for clients who have other, more intermittent, high physical demands such as in-season sports or having to shovel snow which may affect how much rehab exercise a person can do on any given day.
I don’t find RPE as helpful for clients:
- Who tend to overdo it or are lazy
- Who aren’t very good with form and need a lot of cueing
- Or for clients who are more sensitized and don’t have a lot of exercise tolerance
This does not apply to mobility exercises as they are (or at least should be) fairly low intensity.

Alternating sets, circuits (giant sets) and supersets
Alternating sets are similar to supersets but are not quite the same. Circuits, or giant sets as they’re known in the bodybuilding world, are just supersets with more exercises. To illustrate the difference with a couple examples…
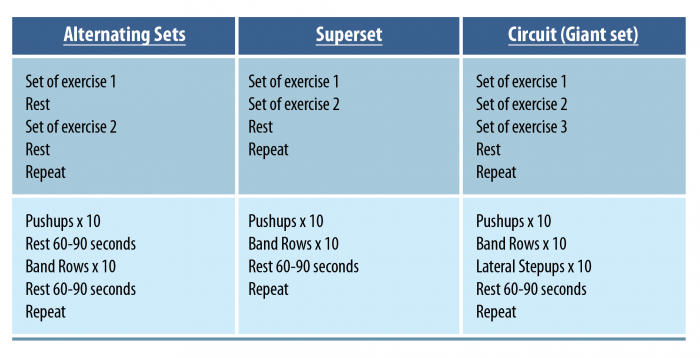
These work good in situations where there are multiple exercises that:
- Work different muscles
- Aren’t super technical and aren’t prone to breakdown when fatigued (I wouldn’t recommend doing these with the vast majority of the big barbell movements)
I even use these with more lower level “traditional rehab” exercises to help clients get rehab done in a short time. These also have added benefits of:
- Making rehab less monotonous
- Getting the heart rate up
Commercial breaks
This is pretty straightforward and just consists of having the client do sets of exercises during commercial breaks of a TV show. It works good for exercises that don’t require any setup or fancy equipment.
That said – due to the popularity of Netflix and other services this technique doesn’t work as well as it did many years ago!
Wrapping Up
Doing exercises to recover from a musculoskeletal pain condition does take time and consistency – but these techniques can help to make exercise programs much more time friendly and improve adherence. For more information on the topics explored in this blog, check out the two masterclasses below:
- Exercise Prescription In Sports Rehab by Dr. Teddy Willsey here
- Exercise Prescription In Aging Adults by Dr. Mariana Wingwood here
Thanks for reading!
Want to learn how to optimise your exercise prescription for older adults?
Dr Mariana Wingood has done a Masterclass lecture series for us on:
“Exercise prescription for aging adults”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!