Lateral Ankle Sprains – To Rehab or to Reconstruct?

‘This is the third time I have rolled my ankle in 7 months. It’s affecting my performance, the club are not going to renew my contract and it’s having a massive impact on my self-confidence and belief… I need to get this surgery done ASAP’
It happens all too often
For those who work in elite level sport, you would have heard the above comments on countless occasions involving catastrophizing thoughts, denial and disbelief.
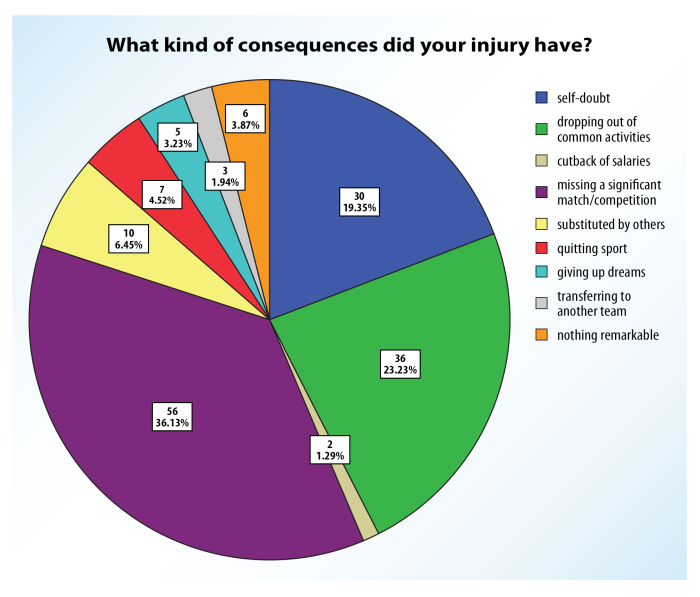
Mittly et al (2016) looked at the potential consequences on patients’ psychology post ankle injuries and alarmingly found that 19.5% of athletes had self-doubt issues and 23.2% dropped out of their common activities.
But why when it comes to ankle sprains, do we as clinicians not pay much attention to a person’s psychology and wellbeing, instead we are engrossed and over-reliant on the bio-medical side of things and only ever concerned about the physical parameters such as, ankle arthrokinematics, vertical jump testing or questionnaires….to name a few! Before we carry on, if you want more detail on all things related to ankle sprain assessment and management, check out Chris Bleakley’s masterclass here.
Granted, the management of elite level athletes differs from a weekend warrior or the general population but the impact of psychology can have a detrimental impact on everyone. From not being able to perform at the highest level on a Saturday afternoon, to not being able to walk to the local shop to grab the daily newspaper…the impact is indisputable!
Clinical viewpoint
While ankle sprains are very common in the physically active population (Roos et al., 2017; Wiersma et al., 2018; Kerr et al., 2022 cited in Gaddi et al., 2022) approximately 25% of adults in the general population have a history of ankle sprain (Baldwin et al., 2017 cited in Gaddi et al., 2022). Unfortunately, in the general population, care for ankle sprains is often limited to symptom management (Bowers et al., 2021; Kosik et al., 2021 cited in Gaddi et al., 2022), and consequently long-term symptoms and physical dysfunction are common following an ankle sprain.
Should we as physios be doing more to help patients understand their ankle pathology? Should we be using more pain science methodologies? Should we encourage patients to make their own informed decisions rather than be influenced by the medical professionals? Is a shared decision making attitude always helpful? Let’s find out what the current literature says regarding lateral ankle sprain management both surgical and non-surgical.
The research phenomenon
Most recently, a systematic review by Gaddi et al (2022) and Altomare et al (2022) found that there was high quality evidence for non-surgical management of acute lateral ankle sprains.
However, the perception of patients is usually that they require surgery to fix the ‘torn ligaments’ and this is usually reinforced by most orthopaedic surgeons and scare tactics are often used which can have a remarkable impact on a patients decision making power and inevitable outcomes. Sometimes, considering a patient’s background noise such as a recent family bereavement, marital issues or even financial trouble rather than mechanical vs functional instability is something that definitely lacks consensus.
Kerkhoffs et al (2007) discussed the surgical versus non-surgical approach for acute injuries of the lateral ligament complex of the ankle and found insufficient evidence in all the RCT’s to confirm the effectiveness of surgical management. They included 20 trials and 2,562 patients.
Approximately ten years on, Al Mohrej et al (2016) concluded that regardless of the severity of ankle sprains, surgery should not be recommended. Most recently, Qi-Liu et al, (2019) compared 834 patients in the surgical group to 930 patients in the non-surgical group and they concluded that surgery may improve the AOFAS outcome score, but the rate of complications was higher and no difference was reported in the incidence of recurrent ankle injury.
The only current paper in the literature that appreciates the power of pain psychology somewhat is the PAASS Framework by Smith et al, (2021) which looks at athlete perception, confidence, reassurance and readiness to return to sport. The importance of obtaining input from the athlete is fundamental in guiding return to sport. It cannot and should not be based entirely on the physical capabilities.

The never ending debate
Ultimately, psychological impairments persist in individuals with a history of ankle sprain. The fear and anxiety to return to sport or any meaningful activity remains evident. Apart from looking at physical parameters, patient reported outcomes and questionnaires can we as clinicians spend a little more time understanding the patient and his/her background like we do with a patient with back or knee pain.
For example, a 14 year old boy who has been suffering domestic violence at home and being bullied at school who plays football to relieve some stress and ends up rolling his ankle. Should we as clinicians be focusing solely on the ankle or plunge deeper into the child’s background and understand why he may have sustained that ankle sprain.
Similarly, a 72 year old female who has been diagnosed with cancer and has recently lost her husband, has no family support trips on a loose rug as her thoughts and emotions were elsewhere. Do we as clinicians focus on the individual’s ankle, or do we explore why she may have suffered the ankle sprain? As always, we need to remember we are not treating JUST an ankle injury. We are treating an ankle connected to a person.
Wrapping up
To sum up, health related quality of life and assessing patient’s priorities, goals, values, expectations and perceived wellbeing, while also encompassing their physical, emotional, psychological, and social status should be paramount when deciding to rehab or reconstruct.
To learn more about the treatment and management of lateral ankle sprains, you can always check out Chris Bleakley’s masterclass here.
Thanks for reading.
Want to get better at treating ankle sprains?
Chris Bleakley has done a Masterclass lecture series for us on:
“Ankle sprain: etiology, diagnosis and rehabilitation”
Try it for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!