Everyone with Heel Pain Does Not Have Plantar Fasciopathy – Just ask Mr. Baxter

The guessing game
How many times have you seen a patient and thought, ‘’I know what the diagnosis is’’ as soon as they point to their heel? Go on, admit it, we’ve all done it!
How many times has a patient told you they have been googling their symptoms and believe they have plantar fasciopathy? Go on, admit it, plenty of times!
Unfortunately, there are heaps of pathologies that masquerade as plantar fasciopathy which we as clinicians need to be well equipped to recognize when we encounter them.
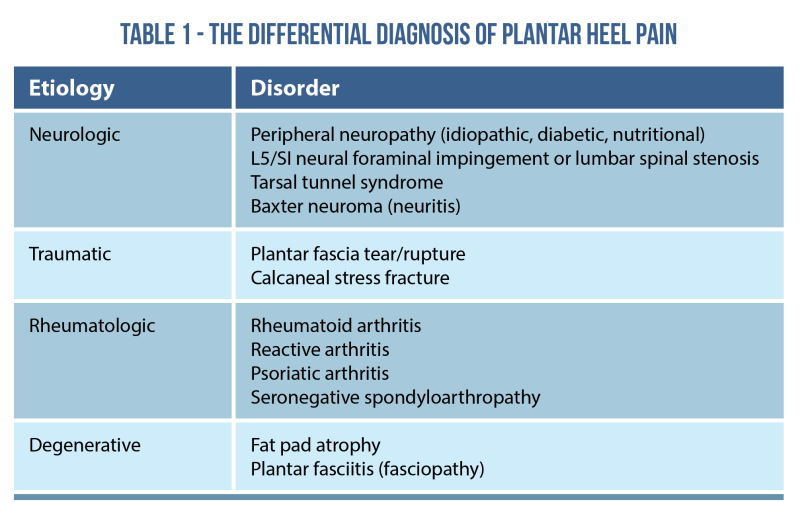
One such differential diagnosis is Baxter’s Nerve Entrapment or Baxter’s Neuropathy. Baxter’s nerve entrapment can often masquerade as plantar fasciopathy, particularly when encountered in active younger patients (1). The differential diagnosis of plantar heel pain is broad and includes plantar fasciopathy, plantar fascia rupture, calcaneal stress fracture, and fat pad disorders such as fat pad atrophy.
Before we get stuck in, check out this masterclass by Dr Henrik Riel to improve your differential diagnosis of heel pain.
The uncommon presentation
Plantar heel pain (PHP) is a common problem among adults. It can lead to severe pain which causes significant disability and impairment of activities of daily living. PHP can be due to local causes such as plantar fasciopathy, referred causes like S1 radiculopathy, or systemic illness like seronegative spondyloarthropathies (SpA) (2).
Compression neuropathies of the foot and ankle occur frequently in athletes and individuals wearing ill-fitting footwear. As compression neuropathies are often misdiagnosed, understanding the musculature and neural distributions within the foot and ankle can ultimately lead to more accurate diagnoses (3).
Baxter’s nerve is the first branch of the lateral plantar nerve. It provides motor innervation to the quadratus plantae, flexor digitorum brevis, and abductor digiti minimi muscles. Also, Baxter’s nerve carries sensory information from the calcaneal periosteum and the long plantar ligament. Baxter’s nerve can be entrapped distally due to tight fascial planes between the abductor hallucis muscle and the quadratus plantae. Another entrapment site is at the anterior aspect of the medial calcaneal tuberosity (as it passes laterally) between the flexor digitorum brevis and quadratus plantae.

The presence of a suspected compressive neuropathy may be confirmed by imaging and/or electromyography, but should be initially evaluated with a focused physical examination. In the case of Baxter neuropathy, the diagnosis is confirmed by magnetic resonance imaging (MRI) demonstrating atrophy of the abductor digiti quinti minimi muscle belly (4).
Mainstay treatment
Physical therapists should be aware of the typical presentation of neural involvement which includes burning, sharp, shooting pain that can be accompanied by weakness and sensory changes. Patients with Baxter’s neuropathy do not have “first-step” pain when getting out of bed in the morning that eases with activity, nor do they have pain when getting up after short intervals of sitting or rest.
With Baxter’s neuropathy, the pain in the heel worsens with activity and builds as the day progresses. Unfortunately, physiotherapy and rehabilitation alone can occasionally not be enough to resolve symptoms. In this instance, an ultrasound guided injection can be considered as they have been proven to be highly accurate when compared to blind injections (5). It is vitally important that after the injection, the patient embarks on a physiotherapy program to ensure the pain does not return.
Potential masqueraders
Neuropathy of the Baxter nerve is described with prevalence between 15–20% in the literature, and is very relevant among the PHP population in general and has been described to be the first cause of PHP with neurological origins. It is recognized that there may be cases of plantar fasciopathy which overlap with Baxter’s nerve entrapment (6).
Case study examples
With all MSK presentations, the clinical history is the most crucial aspect. As clinicians, we must listen to the patient in depth as they are usually telling us the diagnosis. The evaluation of a patient with heel pain should begin with a focused history to elicit the timing, onset, character, location, and intensity of the pain. So put on your critical thinking hats and here are some case studies for you all to ponder over.
- A 26 year old builder presents to you in the clinic and describes falling from a ladder and landing directly on his left heel 8 days ago. No significant medical history. No imaging. No regular medication. He is able to partially weight bear. No neurological deficits but has some purple/black bruising at the base of his heel and lateral ankle. What would you be thinking? Correct, it’s a traumatic injury which would likely be a calcaneal stress fracture and not a Baxter’s neuropathy.
- A 58 year old female teacher presents to you in clinic with 4 months of worsening bilateral heel pain, right worse than left. Her underlying medical conditions include Psoriasis and Crohn’s disease and reports night time pain and AM stiffness around elbows, knees and heels, but better with movement. Takes prednisolone. She reports intermittent numbness/P+N’s under her heels. What would you be thinking in terms of your diagnosis? Precisely, an underlying rheumatological disorder, not a classic Baxter’s neuropathy.
- A 43 year old male patient presents to you after a spike in training volume as he is preparing for the London Marathon. No underlying medical conditions but recently suffering with depression and anxiety due to marital issues. Is taking sertraline. He reports pain and stiffness during the first few steps after waking up. No sensory changes in the feet. He has modified his training load and taken some NSAID’s and has been icing regularly. What would be your diagnosis? Exactly, probably Plantar fasciopathy or maybe Achilles tendinopathy not a true Baxter’s neuropathy.
These case studies highlight the importance of a thorough subjective examinations and use of clinical reasoning to help us with our differential diagnosis when it comes to PHP. Even experienced clinicians can miss these presentations and it’s OK to openly discuss with the patient the potential masqueraders as they will appreciate you taking the time to understand their story and guide them along the best clinical pathway.
Wrapping up
- Not every patient with heel pain has Plantar fasciopathy
- Not every person with heel pain needs soft tissue work, shockwave therapy or orthotics.
- The differentials for heel pain are exhaustive and we as clinicians need to be better at listening to the patient’s story and most importantly validate their ideas, concerns and expectations.
- The foot and ankle is still connected to a person and not just another body part.
If you found this useful, check out the masterclass by Dr. Henrik Riel on diagnosis and managing plantar heel pain here.
Want to become an expert on plantar fasciitis?
Dr Henrik Riel has done a Masterclass lecture series for us!
“Diagnosing and managing plantar heel pain”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Leave a comment (1)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
What are the differences in treatment options between plantar pasciopathy and fat pad atrophy?
Thanks