Two’s Company and Three’s a Crowd: Physiotherapeutic Interventions for Lumbar Spinal Stenosis (LSS)

LSS is an age-related condition associated with anatomical changes towards the lumbar spine. Its prevalence increases with age and is thought to be present in around 45-60% of older adults, yet only a small percentage of these are symptomatic (1,2,3). One of the cardinal features of LSS is neurogenic claudication which develops in extension postures secondary to reduced cross-sectional area of the spinal column and subsequent compression of neurovascular structures (9).
Additionally, crowding around the nerve root and corresponding arterioles results in neuroischaemic pain in the buttocks and lower limb which impedes physical activity. In more advanced cases, sensory and motor deficits can manifest via reduced nerve conduction and venous congestion which has been shown to negatively influence mobility, balance and general health (4).
This blog is going to evaluate the conservative options available for managing LSS. This is of particular importance as current evidence has concluded there is little confidence surgery outperforms non-invasive interventions (5,6). Furthermore, glucocorticoid injections offer no advantage versus anaesthetic alone and have little efficacy for short and long-term benefits respectively (7,8). For further information, see this review by Dr Mary O’Keefe.
Treatment options
Emphasis is focused on improving or stabilising symptoms and although LSS is degenerative in nature, reassuring patients that 33-50% of those with mild-moderate symptoms do improve without surgery (9). More recently, a stepped approach which encourages education and self-management initially, followed by supervised multimodal rehabilitation and psychological interventions are recommended for those who continue to experience symptoms (10). There is a lack of high-quality studies investigating conservative approaches to LSS, yet the overall consensus supports multimodal rehabilitation within a supervised setting (3,12).
Treatment instead should focus on improving general health rather than anatomical changes; as the former is likely to improve symptoms associated with the condition. LSS is a risk factor associated with metabolic syndrome and vascular comorbidities secondary to sedentary behaviour which is driven via neurogenic claudication (12,13). LSS is also a leading cause of disability within the elderly and can reduce walking capacity, quality of life and can lead to depression (14).
Clinicians should therefore educate patients about healthier lifestyle choices and highlight the array of exercises available. Also, by helping facilitate engagement towards these interventions, it may improve self-efficacy with managing LSS whilst potentially having a concomitant effect on tempering degenerative changes of the lumbar and attenuating progression of the condition (15).
Aerobic Exercise
Considering alternative forms which do not exacerbate neurogenic claudication from walking has been shown to improve pain, disability, mental health and reduce pharmacological intake (16). Partial body weight walking, cycling and aquatics has been shown to decrease axial load on the spine and help with pain and disability (17). The former often requires specialist equipment such as an anti-gravity treadmill which is not readily available in most clinics, whereas the latter are more feasible.
Hydrotherapy
The buoyancy and resistance of the water will reduce load placed through the spine whilst strengthening the lower-limb respectively and provides greater short-term improvements in pain and function (18). Options include, swimming, walking, light jogging or utilising classes like water aerobics which provide a social dynamic for the patient respectively.

Cycling
An intervention which has illustrated promising results for LSS. The rationale is that a flexed sitting posture increases cross sectional area around the spinal column, reducing neurovascular compression and exercise-induced ischaemia of the cauda equina (19). Programmes involving 60 to 90 minutes each week over 4 months improved walking distance, oxygen uptake and reduced the need for surgery (20). The theory is that by improving cardiovascular and circulatory health, it may attenuate the ischaemic symptoms associated with LSS (3). Cycling also improved radicular symptoms associated with nerve compression (21, 10).
Strengthening & motor control
Physiotherapy has been a longstanding staple for LSS, with practitioners favouring flexion-based exercises (22). This is an approach I also tend to adopt during early rehab as part of activity modification away from the irritable stimulus. Extension-based exercises are then integrated for graded exposure into upright postures to improve tolerance, confidence and reduce kinesiophobia in these positions. Unfortunately, this is anecdotal and from clinical experience, so I am fully prepared to take a pasting from the twitter gurus, or perhaps I should publish a study? See below for some exercise ideas.

Figure 1
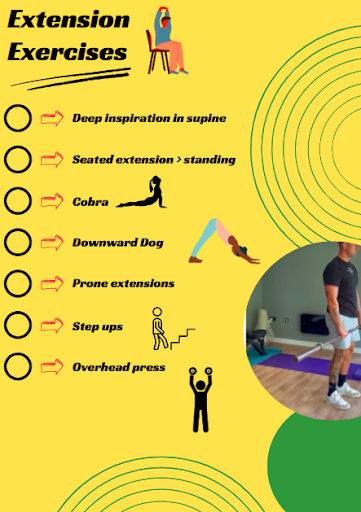
Figure 2
Balance exercises
Impairments in balance are common secondary to neurogenic claudication and because of a triad of features;
- Sensory deficits.
- Muscle weakness.
- Postural instability.
This negatively influences nerve conduction, physical inactivity and creates excessive trunk flexion (17). Consequently, this may place LSS patients under a greater predisposition towards falls; something that already occurs in approximately 33% of elderly patients each year (23). I like to incorporate resistance training in closed chain positions whilst progressively challenging balance by altering the base of support and including dynamic options. This is because interventions which target both have been shown to reduce falls in older adults (23). Examples include;
- Static – overhead press, lateral raises (you can do these with narrow or tandem stance)
- Staggered Sit-to-stand / split squat / clean and press
- Pallof press / cable oblique twists
- Dynamic – step ups / multi-directional lunges
- Overhead carries
- Farmers walks
Exercise prescription
When looking at exercise prescription for this demographic of patients, I personally like to keep things simple and follow the World Health Organisation guidelines for physical activity in older adults (24). Especially considering a large subset of this population are already fairly sedentary, see below;

Figure 3
Outcome measures
This is not an exhaustive list, but some useful options to consider for LSS when looking to assess the effectiveness of your interventions alongside patient satisfaction (25).
- Oswestry Disability Index
- Modified Romberg Test
- Zurich Claudication Questionnaire
- Six minute walk test
Wrapping up
To conclude, the evidence surrounding physiotherapeutic interventions for LSS is sparse and of low quality, but is a topic being investigated thoroughly given its rising prevalence due to an ageing population. Currently, multimodal and supervised programmes appear to be more efficacious and therapists should reassure patients about the favourable prognosis, whilst highlighting an array of exercise options available to choose from to improve overall health and successful self-management.
📚 Stay on the cutting edge of physio research!
📆 Every month our team of experts break down clinically relevant research into five-minute summaries that you can immediately apply in the clinic.
🙏🏻 Try our Research Reviews for free now for 7 days!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!