Returning to Running Post Injury: Part 2 – High Speed running

Ok, so you have a patient in front of you with an acute lower limb injury. As in part 1, we’ve seen a mismatch in the load vs capacity relationship. Although this time a tissue has acutely failed. How confident are you at guiding your patient from day 1 to returning to high intensity running performance?
My hope here is that this blog can be a guide for you to lean on when you next face this challenge in the clinic.
In this blog I am going to cover:
- The spectrum of intensity on the gait rehab continuum
- Overloading gait mechanics drills
- Using Maximal Aerobic Speed (MAS) in rehab (including calculations and programming parameters)
- Anaerobic speed reserve (ASR) considerations for late stage rehab
- High speed running and sprints
These concepts are very pragmatic and easily applied in the field / court sport athlete context due to the demands of the tasks they need to return to. However, they could also have some utility in the context of your endurance athlete with an overuse injury as well, as per part 1.
1) Gait rehab continuum
From day dot where you have a patient in front of you, we should be thinking of what their goal level of running activity is, what positions they need to achieve for that, and how this will require their tissues to be loaded. Therefore, gait retraining / restoration is always front of mind here.
At one end of our spectrum we have non-weight bearing with mobility aids, and at the other we have maximal velocity sprinting. Parallel to this, we also have change of direction and agility continuums and loaded gait mechanics drills, that can be introduced once safe walking balance and weight shift are achieved.
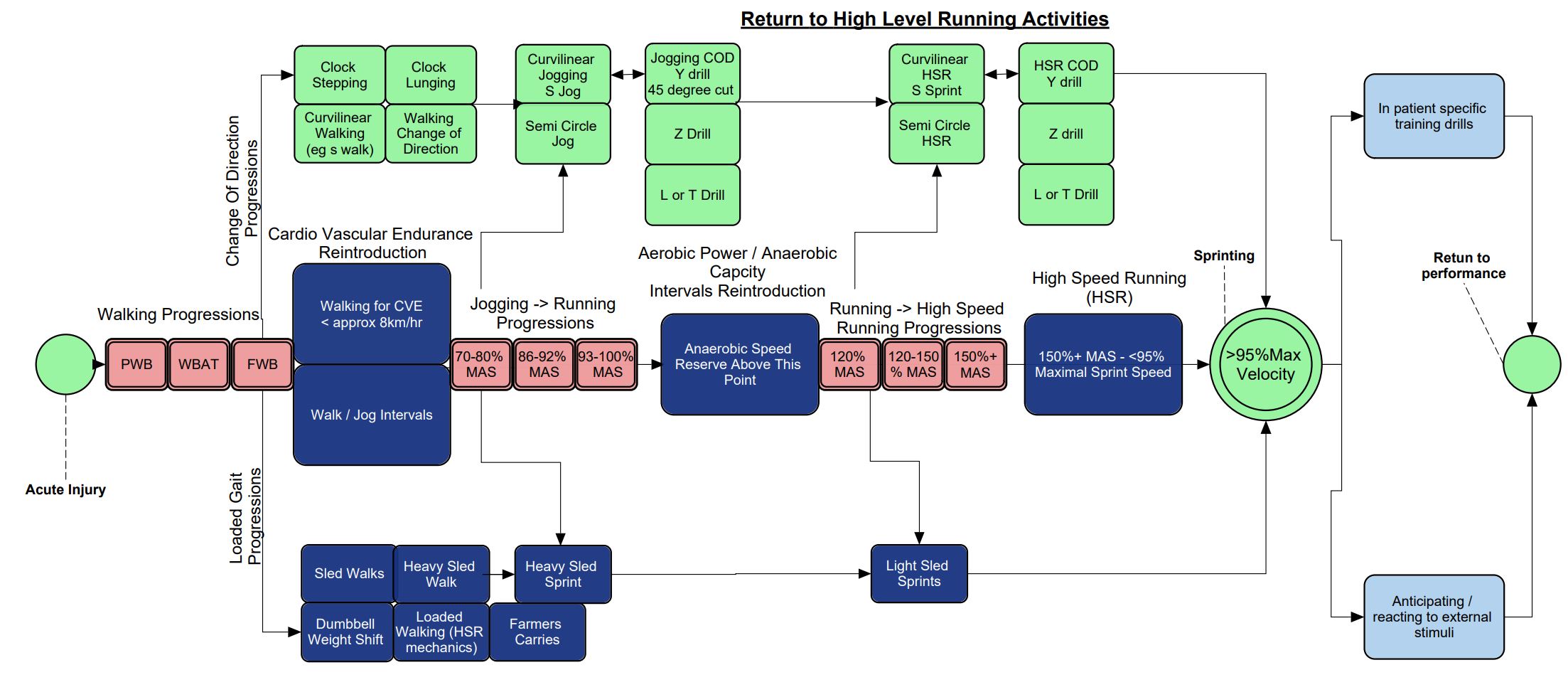
Figure 1
I like to linearly progress through this continuum, with some individual differences based on goals and objective response. This ensures that the tissues of the lower limb have successfully been exposed to loading and built tolerance in order to progress to more difficult tasks. This way you can also definitively outline to a patient where they are in relation to their running related goal, and what they need to be exposed to in the coming phase of rehab.
2) Overloading gait mechanics drills
Often our athletes or weekend warriors, who have acutely injured themselves in a sporting context, are used to running being a high intensity repeated task.
Enter loaded carries and sleds. These are some of my favorite ways to expose a patient to those same intensities and goal positions. The option of varying the load (as you would in traditional resistance training, or speed in running drills) allows a clinician to control the impulse experienced by the tissue. This allows us to apply a load that is specific to the task of gait and provide a progressive overload stimulus for adaptation.
Below is a video of some of my favorite drills and their use:
Note for performance:
A sled at 20% body weight or less can improve acceleration / sprint speed. This is because the stimulus is still similar on the force velocity curve to that of sprinting. On the other hand, relatively heavy sleds require longer impulse and can often be tolerated better earlier in rehab but transfer less to performance (1).
On a final note, I love the ability to have time to coach foot and ankle stiffness in the context of gait that sleds allow compared to other running drills. This will be vital later in higher speed running.
3) MAS
Previously in part 1, I showed you how to run a MAS test. Here, I’m going to show you what to actually do with the result. Often our athletes have results of these, in the way of a time trial, or a beep test that they performed pre-injury. This is a good baseline to be used in the return to play conversation and goal setting. This is due to the risk of injury from low cardiovascular fitness when compared to peers (2,5). So getting back to these numbers could be important.
Example 1: How to use a beep test to get a target MAS (3,4,5)
From the beep test – E.g. the patient achieved a 10.3 (10 levels 3 shuttles) before failing.
- MAS (km/h) = Final Shuttle Speed (km/h) * 1.34 –2.86
- Table of speeds accessed here: https://www.topendsports.com/testing/beep-table.htm
- For a 10.3 beep test the final speed is (13km/hr)
- MAS = 13 * 1.34 – 2.86 = 14.56km/hr (4m/s)
- Usually m/s easiest value for interpretation and prescription
Example 2: How to use a continual running test (e.g. 1.2km time trial) to get a target MAS (4)
- 1.2km time trial (1200m)
- Took 5 minutes (300sec) to complete
- 1200/300 = 4m/s
Alternatively, you could conduct a MAS test yourself depending on the length of rehab, deconditioning and pain responses. For prescription purposes, always try to match a patients running prescription to where they are objectively from a tissue capacity standpoint. Only start touching higher intensity MAS (100%+) running as the patient nears pre-injury levels and Limb Symmetry Index (LSI) is normalising. This will minimise compensatory movement patterns from becoming engrained post injury. Compensation will occur due to exposure to a stimulus above tissue capabilities (17, 18).
Clinical Pearls for Prescription
Based on what intensities your patient can run, here is a guide on how to build your program:
- <70% MAS LISS (low intensity steady state). Recovery runs up to 30+ minutes or rest between intervals.
- 70-80% MAS aerobic threshold. MISS (moderate intensity steady state) predominantly aerobic. 10-30min runs. Usually too intense to be used as rest intervals.
- 86-92% MAS HISS (high intensity steady state) Anaerobic threshold. Starting to require more anaerobic glycolysis for energy >6-8mins (5,6).
- 93-100% MAS (aerobic power training). This is a point of running where efforts of maximal intent can last <8 mins and correlates with VO2max. Usually performed in intervals 2-1:1 work:rest <60 seconds / effort (5,7)
- 120% MAS. MIIT (medium intensity interval training) Anaerobic capacity / aerobic power training. 2-1:1 work:rest <30 seconds / effort
- >120-150% MAS. HIIT (high intensity interval training) Anaerobic power training. 1:1-2 work:rest 15-30 sec / effort.
- 150+% MAS. SIT (Sprint interval training / Repeated Sprint Ability) ATP -PC capacity. Anaerobic power training. 1:2-6 work:rest <15sec / effort (5, 6)
Most of the time near maximal or supramaximal MAS running is done in blocks of 10 minutes per session (5).
4) Anaerobic Speed Reserve (ASR)
This is an emerging area of research regarding its impact on physical performance, load management and possibly injury. Essentially, it is the zone of high intensity running that exists between MAS and maximal velocity sprinting.

Conditioning work in the ASR, will confer a high training stress per unit of training time. This can be important for training load monitoring and ensuring smart incremental volume load targets of ASR running. This build up is critical though as most field sport activities occur in this range between MAS and top speed. So the main takeaway is, you need to ensure your athlete has done enough of this running to be prepared for sport without introducing a potentially risky training load spike (8,9,10).
5) Sprinting
Maximal sprinting is a highly demanding and biomechanically specific task (>98% top speed) compared to high speed running (<95% top speed) (11-14). Therefore, I recommend only introducing maximal speed work for the purpose of improving speed when LSI and relative strength compared to pre-injury are normalised. High speed running (<95%) however can be built in earlier with the MAS work, within pain limits (15).
My stance on this has changed since looking deeper into the dynamic systems theory literature, where we can see the body compensate in many circumstances to achieve a task (17,18). Previously, I was an advocate for graded exposure approach of building from low to maximal velocity running, but now I’m using a criteria of normalising LSI first. My reasoning is that I want to return the athlete to sprinting with the same capabilities as pre-injury, rather than compromise and develop less optimal motor patterns that may have to be retrained once the injured tissue can tolerate the forces required (17,18).
With sprinting here are some good volume landmarks to set your total distance / session:
Acceleration (6, 12, 13)
Length / rep: 5-30m
Total distance / workout: <350m
Rest between efforts: 1:6-10+ work : rest
Frequency / week: 2
Sub Maximal Velocity <95% (7, 12,14)
Length / rep: 40-100m
Total distance / workout <500m
Rest between efforts: 1:6-10+ work : rest
Frequency / week: 2
Maximal Velocity >98%
Length / rep: 40-60m
Total distance / workout <150m
Rest between efforts: >2mins
Frequency / week: 2 (7, 12,14)
Wrapping Up
So there you have it. Now no matter what running related injury you have in front of you, you will have strategies to guide your patient to success in their high level running goals. If you want to learn more about running related rehab, then check out Dr Rich Willy’s Masterclass Restoring Load Capacity in the Injured Runner.
Want to learn more about running injuries?
Rich Willy has done a Masterclass lecture series for us on:
“Restoring load capacity in the injured runner”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!