
Hi everyone!
I just wanted to develop on an idea I have recently had and you may have seen it in one of my recent tweets here:
https://twitter.com/ashjamesphysio/status/960546683288543232
It was based on a general observation that the patients I see who are able to return either back to work or to the activities they enjoy have 3 consistent traits. I found that they all are:
Optimistic, Active and Resilient.
This is where the OAR concept came from. What I wanted to do with this blog was elaborate on each of these ideas and demonstrate the underlying evidence base in relation to pain and disability.
Optimism
A player I worked with as a physio with Welsh Rugby used to give advice to any of the injured players, he used to talk about being a ‘Coke Can’ not a ‘Coke Can’t’. Apart from continuing to make me laugh to this day, it turns out that he was not only funny, but extremely evidence based!
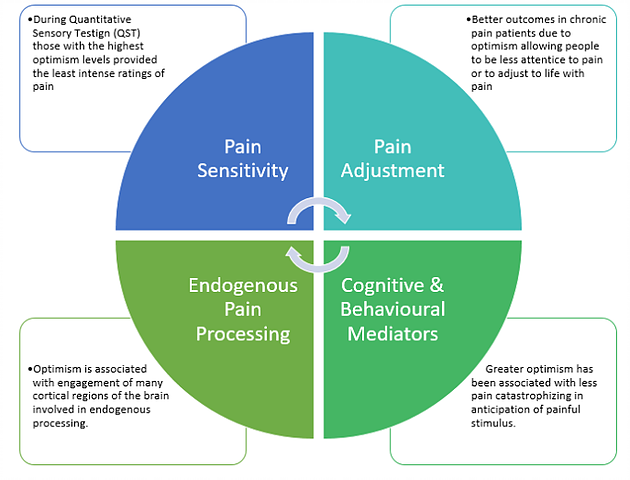
There are loads great papers on optimism and pain, some of which are here:
http://www.thblack.com/links/RSD/Pain2013_154_53_optimismLowersPain.pdf
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3935764/pdf/nihms550889.pdf
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3592576/pdf/nihms426985.pdf
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2921311/pdf/PE_4_5_35.pdf
While they are all on slightly differing topics they all have similar themes. Optimism seems to have some common traits in relation to pain.
Active
I’m not sure I am going to spend too much time here as I think as physiotherapists our underpinning knowledge in how exercise and physical activity is beneficial to patients is relatively sound. If you would like to follow some real influential figures in this arena on social media, I would point you in the direction of a few people. For all things upper limb; Adam Meakins (@AdamMeakins) and his mantra of ‘You can’t go wrong with getting strong’, as well as Jo Gibson (@ShoulderGeek1) who really goes into the evidence of ‘Brain Rich Rehab’ when talking about the shoulder. Ben Cormack (@CorKinetic) runs a great training course which he recently delivered part of to myself and other clinicians I work with. He has some great insight into exercise and its effect on pain as well as how to maximise adherence.
In terms of evidence there is masses out there but one review from last year that nicely lay out that exercise has the strongest effect on reducing musculoskeletal pain in primary care.
You can find the paper here:
http://journals.plos.org/plosone/article/file?id=10.1371/journal.pone.0178621&type=printable
…and a summary of its findings here:
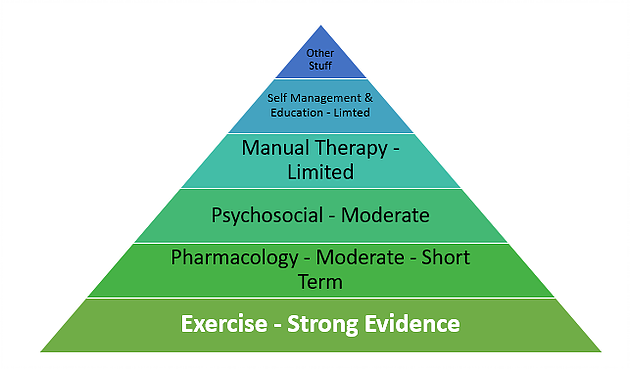
The benefits of being physically active have been laid out in many different ways which do not need regurgitating here, but what I would like to ponder on is what links all 3 of my OAR concepts, and therefore how can being optimistic help someone to be active.
It turns out that highly active people also tend to be more optimistic
Or, are highly optimistic people more physically active? It seems we have a chicken and egg scenario when it comes to these first 2 aspects but in all honesty does it matter? What I take from it is if I can develop some optimism in some of my more pessimistic patients, could that have a knock on effect of making them more physically active? I think what the data shows us that this is probably likely.
In the therapeutic sense Greg Lehman (@GregLehman) talks about being a ‘Movement Optimist’. I really liked that term when I first heard him use it and I think it’s something we can all take forward with our patients. Trying to instil the notion that no movement is inherently bad and having the ability to move in lots of different ways gives you lots of different movement options and will have a protective affect against injury. Being a movement optimist will help to build a patient’s resiliency!
In terms of resiliency however, there may be some benefit in thinking not just locally in our exercise prescription, whether that be the knee, the shoulder or the back, or even in terms of whole physiological benefits but to think in a much broader context…..
[banner-ab-testing]
Resilience
This really is one of my favorite topics and is something that the first 2 components of my OAR contribute towards developing. It fascinates me how 2 different people react completely differently to the same stressors. A person’s resilience is based on both internal and external factors. Resilience depends not just on one’s internal ability to manage and respond but also to the external social constructs and contexts that individual finds themselves in.
If we start at the neurobiological level, there are some fascinating studies out there that discuss the neuroendocrine response to stressors in relation to resilience. When an individual is exposed to a high stress situation (such as a military operation) the sympathetic nervous system is strongly activated and neuropeptide Y (NPY) and galanin are released along with norepinephrine to maintain the sympathetic nervous system in an optimal range. Special Forces combat soldiers have demonstrated they have a higher production on NPY to maintain this optimal range when compared to veterans suffering from PTSD for example. This notion of an ‘optimal range’ seems to be the main neuroendocrine basis for the explanation of differing resilience levels.
This is all well and good but is any of it modifiable from a clinical perspective? What can we do to improve someone’s neuroendocrine response to stressors both physical and psychological? One thing that can mediate this response, which fits in really well with our biopsychosocial approach, is the level of ‘social support’ an individual has. This can vary based on lots of factors including age – an individual’s social support in early adolescence for example seems to have a larger affect over resilience than in later adolescence. But in human studies done in a laboratory setting, those exposed to low social support have demonstrated negative neuroendocrine and physiological responses. Going back to the points made in the activity section then, when thinking about prescribing physical activity for patients, we should be considering not just the local effects of the exercise itself but what social context is it being performed in. Should we consider placing those who seem the least resilient into physical activities that will help improve their social support network? I would argue this would be an excellent idea for their long term health and go some way in improving resilience.
The reference for some of the above points are taken from here:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2921311/pdf/PE_4_5_35.pdf
(Thanks to Derek Griffin (@DerekGriffin86) for pointing me towards the work of Prof Stephen Southwick).
To finish I want to just briefly touch on the 3 primary classes of outcomes, namely:
-
Recovery
-
Sustainability
-
Growth
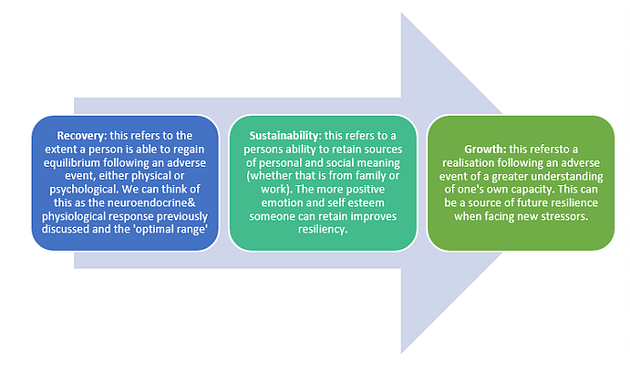
Again the reference to these ideas are much more eloquently put here:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4899321/pdf/nihms195724.pdf
To wrap up I think the imagery of providing patient with an OAR can be a powerful one. The image of being lost on a lonely ocean with no way out can be a very real feeling for some of our patients, particularly those in chronic pain. Providing a route to gaining OAR’s and having the ability to either row themselves out of the abyss or simply beat the s**t out of their pain with the OAR can be empowering!
The simple messages of Optimism, Activity and Resilience has some great evidence behind it with the crooks of it being it provides patients with better coping strategies in the face of pain and a route to growth and development after.
If long term health is what we are after these are traits we must try to instill in all of our patient.
As always thanks for reading,
Ash
This was originally posted on Ashley James’s website. You can click here to read more blogs from them.
Want to master behaviour change?
Dr Serena Simmons has done a Masterclass lecture series for us!
“Behaviour Change in Clinical Practice: A Physio’s Guide to Psychology”
You can try Masterclass for FREE now with our 7-day trial!

Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!