
First it was tendinitis, then tendinosis, now tendinopathy…
First eccentrics were the go-to, then isometrics, now…?
With conflicting research, it seems the only thing that we know for sure is that tendinopathy is challenging to treat.
To simplify what can feel like an incredibly complex topic, in this blog we’ll take you through the 6 Rules to Successfully Rehab Any Tendinopathy.
RULE #1 – Don’t rest completely
Rest isn’t always best – especially when it comes to tendinopathies (1).
This is why the first step in any successful tendinopathy must be to determine whether the patient is over or underloaded. The answer to the following questions should dictate your initial treatment plan:
Can we start to load them immediately?
or
Do they require relative rest?
(Note relative rest, and not absolute rest was mentioned as relative rest is a much more effective strategy to accelerate tendinopathy healing)
More often than not, patients seek treatment for tendon related pain in the midst of a flare-up. This means reducing load is important, but only in the initial stages. We can’t cease load completely for extended periods or we risk underloading the tendon (1).
The goal is simply to reduce the aggravation as a result of the flare up, while returning to graded exposure as tolerated. This allows the tendon to adapt to loads and adequately recover.
Remember: Rest DOES NOT improve tendons long term
RULE #2 – Do progressively load the tendon
Tendinopathy is known as a failed healing response to loading.
Therefore, to change the tendon’s loading response, we must strengthen it through progressive overload. To progressively (but not excessively) overload a tendon, we need to consider how to manipulate the load.
The 3 key variables (as discussed in Dr Seth O’Neill’s Masterclass) are:
- Intensity
- Volume
- Frequency
To determine where to start, it helps to look at the research. The majority of the evidence suggests that heavy slow resistance (HSR) training is the best strategy for tendon rehabilitation (2). The effectiveness of HSR is likely, at least in part, due to the high physical load but minimal shock loading applied to the tendon.
When compared to isometric loading, HSR has demonstrated better client outcomes (2). However, eccentric loading also has a lot of evidence suggesting training benefits over traditional concentric and eccentric training (3). Taking both of these into consideration, both HSR and eccentrics studies utilised heavy (> 75%) loading strategies, so ensuring the resistance is heavy is important.
As tendon healing progresses, we must continue to load it to cope with greater demands. As proposed in this Masterclass by Dr Seth O’Neill, to progressively overload a tendon effectively, the rehab pathway should look something like this:
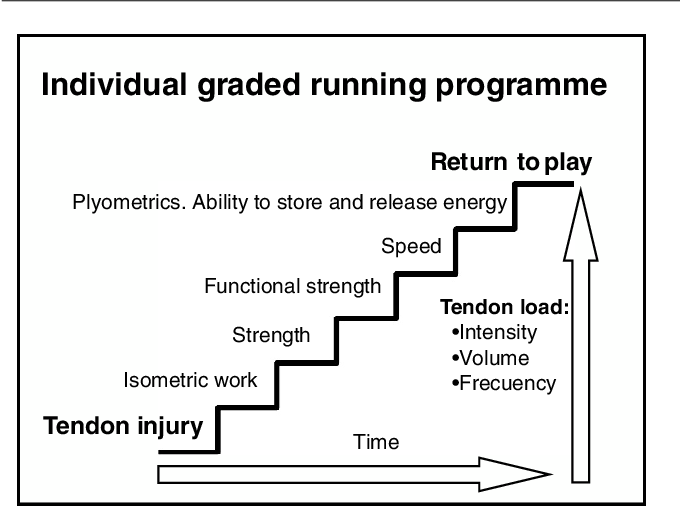
Remember: Tendons LOVE load
RULE #3 – Don’t completely avoid pain
Pain should not be completely avoided when it comes to tendon rehab. Avoiding pain often results in an underloaded tendon and can delay or prevent full tendon healing. The Pain (and activity) Modification Scale is an excellent visual depiction, often used in practice, to help clients understand what pain is and is not okay (1).

To summarize this diagram, we ideally want to stay below a 4 to continue training at the same intensity. A 4 to 5 (or sometimes 6) is deemed as ‘proceed with caution’, where reducing, not ceasing exercise is recommended and anything above a 6 is overloading and exercise should be stopped. Additionally, it is recommended that pain does not increase during or in the 48 hours post exercise by more than 2 points from pre-exercise pain levels (1).
Empowering clients to monitor their own pain levels and adjust accordingly is imperative to self-identify if their training session was too much, too little or just right. Failure to do so results in poorly rehabilitated tendons.
We also know that kinesiophobia is often a result of client’s not understanding their pain. As a result, successful tendon pain management must include education surrounding pain not always equating to pathology, functional capacity or the success of their tendon’s rehab (4).
Remember: Some pain is OK during tendon rehab

RULE #4 – Do set realistic timeframes
Tendon healing takes time and focused effort. Research tells us tendinopathies need a minimum of 12 weeks of consistent loading to show sufficient healing. Therefore, it is important that we encourage continuation of rehabilitation that is progressive in nature. Where rehab is inconsistently loaded and/or non-progressive, tendon healing is unlikely to occur.
While clients love timelines, it’s important to ensure they aren’t married to them. The tendon’s functional capacity and improvements are dependent on the tendon’s healing response and response to actual tendon loading, not arbitrary timeframes. Progress markers and consistency should be emphasized, while education on how loading changes may impact their rehab time frames must be discussed.
Remember: Tendon healing takes time
RULE #5 – Do use isometrics prior to exercise (If they provide pain relief)
Isometrics used to be the gold standard of tendon rehab (Heck, I even did them 15 years ago when I was diagnosed as a teenager with patella tendinopathy).
However, new research has identified that isometrics are only sometimes beneficial for temporary pain relief, with a caveat. They must be performed with at least 80% Max Voluntary Contraction (MVC) to be effective (5). Unfortunately, more often than not, clients are chronically found to be underloading their isometrics.
Isometrics don’t help everyone. With that being said, it may be useful to trial them. Even at 80% MVC, they’re very low impact, and if they can provide temporary pain relief for clients, it’s a great ‘buy-in’ strategy at the very least (5).
Start by prescribing isometrics as part of their “prehab” exercises (5 x 45s with 2 min rest is what the literature states – however anecdotally, I find 3 sets can often minimize pain while also being more time efficient) (5). This allows those clients who do benefit from isometrics, a method of reducing their in-session discomfort. This can be done in the latter stages of rehab and is a great way to continue to maintain a level of consistent tendon loading.
Remember: Isometrics are only sometimes effective
RULE #6 – Don’t compress or stretch the tendon
Healthy tendons are also stiff (and not stretchy) tendons. When we unnecessarily stretch them, we reduce their capacity to transmit forces, which is one of their main roles. Irritable tendons therefore hate compressive forces. This means we should be avoiding positions that cause the tendon to stretch or become taut (1).

Ask yourself this:
What positions does the tendon get stretched and compressed in?
For example with the achilles tendon, it is stretched when we are in dorsiflexion and often compressed as a result of high top shoes digging into the posterior lower calf through direct pressure. This also means massaging, whereby applying direct pressure to an aggravated tendon is a no-go.
Remember: Tendons HATE compression
Wrapping up
While it should be noted that there are differences between tendinopathies in rehab, these 6 Rules can be applied to all tendons to fast-track your tendon rehab success!
If you found this useful and want to learn more about the practical applications of tendinopathy treatment, then check out this great Masterclass by Dr Seth O’Neill.
Want to learn more about tendinopathy?
Dr Seth O’Neill has done a Masterclass lecture series for us on:
“Managing Lower Limb Tendinopathy”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!