
Outside of the acute capsular and ligamentous trauma setting, posterolateral knee pain can be a bit of a ‘No Man’s Land’ pathoanatomically.
In the same vein as ‘anterior knee pain’, here are some conditions to bear in mind if your patient’s symptoms are puzzling you. This is not an exhaustive list, and if you’d like more information on assessing and managing anterior knee pain, be sure to check out Claire Patella’s Masterclass on Patellofemoral Pain.
Biceps femoris tendinopathy
Commonly seen in explosive activity (e.g. sprinters).
Presents with reduced sprint performance and power output; pain on striding out, fast walk and acceleration.
Diffuse aching around posterolateral knee; stiffens with inactivity and then warms up.
Can radiate proximal and distal to fibula head
Ultrasound image – distal biceps femoris (transverse)
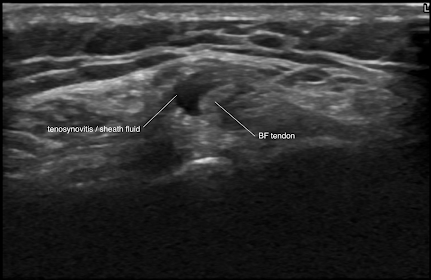
Figure 1
Exam
- Reduced strength and pain provocation on hamstring testing with lateral hamstring bias (e.g. in prone with tibial external rotation).
- Pain on single Leg Romanian Deadlift / arabesque and single leg bridge.
- Tender at fibula insertion – but not a reliable sign.
Popliteus tendon injury
Acutely can occur with pivot and twist mechanism, ‘pop’ mimicking an LCL or ACL tear, but no instability symptoms and the patient often remains functional.
Chronic tendinopathy cases present with aching symptoms radiating from posterior around lateral joint line – seen in overzealous post op ACL rehabilitation, martial arts, judo.
Ultrasound images – popliteus tendon at popliteal hiatus (longitudinal lateral joint line)
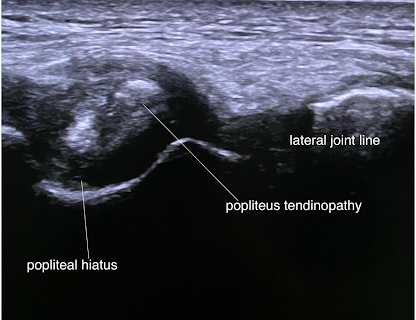
Figure 2
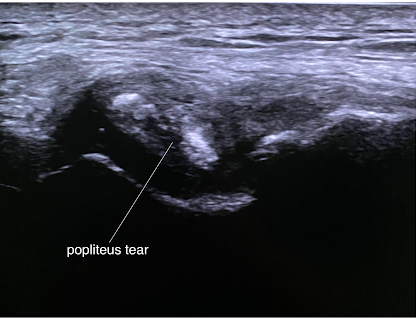
Figure 3
Exam
- Occasionally tenderness focally at lateral joint line and into popliteal hiatus.
- Pain and weakness on resisted knee flexion in prone with tibial external rotation bias; also resisted tibial rotation in 90o knee flexion.
- When popliteus muscle is irritable, patients can describe discomfort or ‘block’ on passive overpressure into flexion and also noted on deep squat. Can mimic meniscal pathology.
Parameniscal cyst
These guys pop up all around the knee secondary to a meniscal tear (think anterior knee pain). If posterior, they can cause space occupying discomfort on flexion.
Figure 4 shows a posterior horn lateral meniscal cyst compressing the common peroneal nerve (CPN) causing insidious radiating neuropathic symptoms into distal lateral shin, ankle and foot.
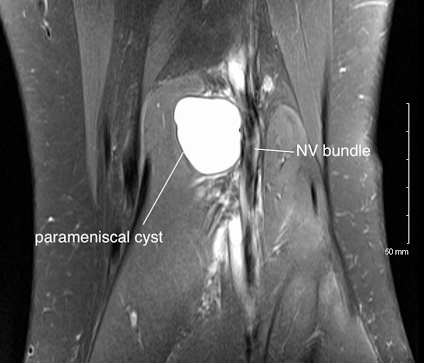
Figure 4
Exam
- Fullness in popliteal fossa if large enough – may feel like a Bakers cyst but more lateral.
- Loss of passive ROM into flexion and squat.
- Effusion related to the meniscal tear and battery of meniscal tests variably provocative.
- May have positive straight leg raise neural tension testing with a CPN bias.
- Neurological assessment may reveal weakness into eversion / dorsiflexion and possible sensory loss lateral into the shin, ankle and dorsal foot.
Superior tibiofibular joint
This is under-appreciated as a source of posterolateral knee pain – I see 4-5 of these a year and are misdiagnosed as ITB overload, lateral compartment pathology or even lateral compartment exertional compartment syndrome.
These can become degenerate, inflamed and effused.
Mechanism of injury typically involves deep knee flexion and rotational activity causing shear and torque effect on the superior tibiofibular joint (STF). Commonly occurs in dancers, gymnastics, powerlifters, as well as high impact and jumping based activity.
Ultrasound images – STF (longitudinal images)
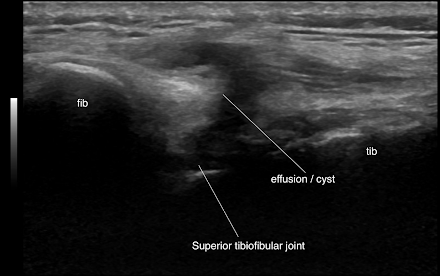
Figure 5
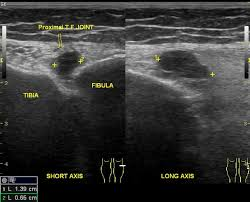
Figure 6
Exam
- Focal swelling (especially if cyst formation) or ‘bony’ deformity at the STF joint.
- Painful and stiff on AP glide (or overly lax) and remember to compare with the contralateral side.
- Pain on dynamic deep squat and Thessaly test.
- Lateral hamstring loading may provoke pain due to shear effect on the fibula head.
- Pain often radiates into lateral shin distally to confuse the clinical picture.
Bony exostoses (benign outgrowth)
Surprisingly common around the knee and the majority are asymptomatic and go unnoticed – but if in the wrong place or large enough, they can cause compressive mischief!
Patients may have a hard block on functional ROM (e.g. squat, kneeling which insidiously progresses).
They can cause local irritation of soft tissues (e.g. hamstring muscle / tendon) or may have progressive neural compressive symptoms.
CT image – sagittal posterolateral knee large exostosis

Figure 7
In the below clip, we can see a large posterior femoral exostosis causing sciatic nerve irritation on dynamic hamstring contraction, triggering distal posterior thigh pain into lateral knee and lower leg.
Treatment? Excise it! But, make sure it’s the cause – it’s prudent to get nerve conduction studies and MRI lumbar spine.
Static image of video
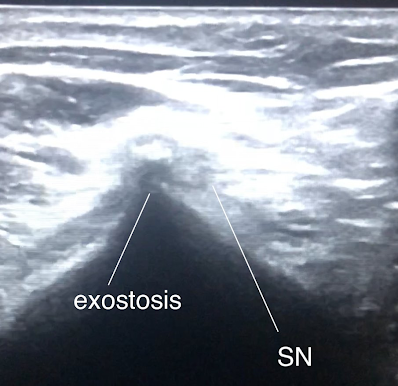
Figure 8
MRI (corresponding image) – axial distal posterior femur
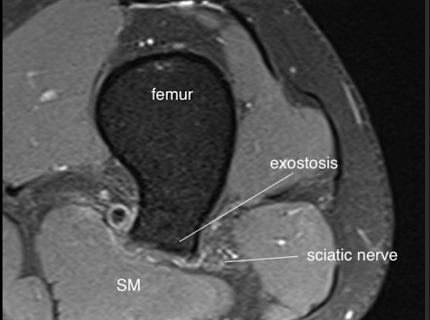
Figure 9
Fabella (lateral gastrocnemius sesamoid bone)
A common incidental anatomical finding and typically asymptomatic.
However, a small handful do cause problems such as local soft tissue inflammation under repetitive loading and compression (e.g. cyclists)
Can also cause irritation of common peroneal nerve (CPN); the result is posterolateral radiating pain into the lower leg, typically neuropathic in nature.
Image – intra-operative exploration of local soft tissues and excision of fabella – CPN seen tied (yellow) and protected
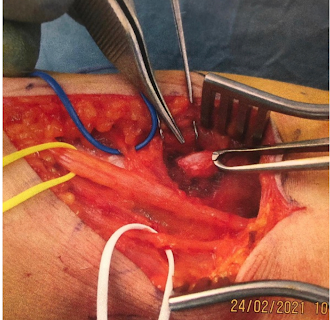
Figure 10 (provided with patients consent)
Ultrasound – CPN in proximity to fabella (transverse)
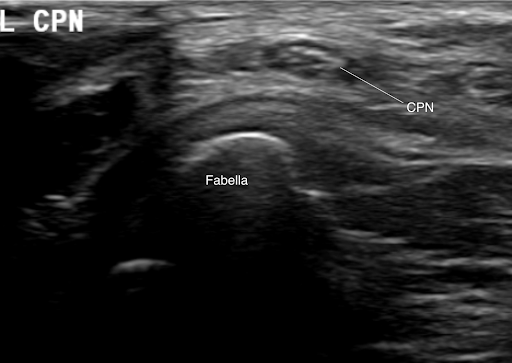
Figure 11
Exam
- Hard smooth bony lump felt on palpation through proximal lateral gastrocnemius with tenderness into and locally around fabella.
- Tinel’s test around the immediate fabella region may provoke neuropathic symptoms distally.
- Lateral hamstring loading may provoke symptoms.
- Variable positive neural tension testing.
- It can be challenging to reproduce symptoms on the couch! It may need sports provocation pre appointment or in-house exercise challenge then reassessment.
Finally – radicular
Pathology at the lumbar nerve root level has a hugely variable clinical presentation – although not classical, it can cause posterolateral knee pain – sciatic pain is not always ‘text book’.
Always think about clearing the lumbar spine in lower limb presentations.

Figure 12 (1)
Worthy mentions
Some other conditions not outlined in this blog but are worth mentioning include the following:
- Posterior horn lateral meniscal tear
- PCL insufficiency
- Atypical ITB compression syndrome
- Distal femoral / proximal tibial metaphyseal bone tumour
Wrapping up
This blog outlined uncommon causes of posterolateral knee pain and I hope it helps you with your management of these patients. If you want to learn more about assessing and managing anterior knee pain, check out Claire Patella’s Masterclass on Patellofemoral Pain.
Want to learn more about anterior knee pain?
Claire Patella has done a Masterclass lecture series for us on:
“Patellofemoral pain”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Leave a comment (1)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Thank you so much. Great summary of uncommon causes of the posterolateral knee Sx.