Manipulating Range of Movement in Rehab

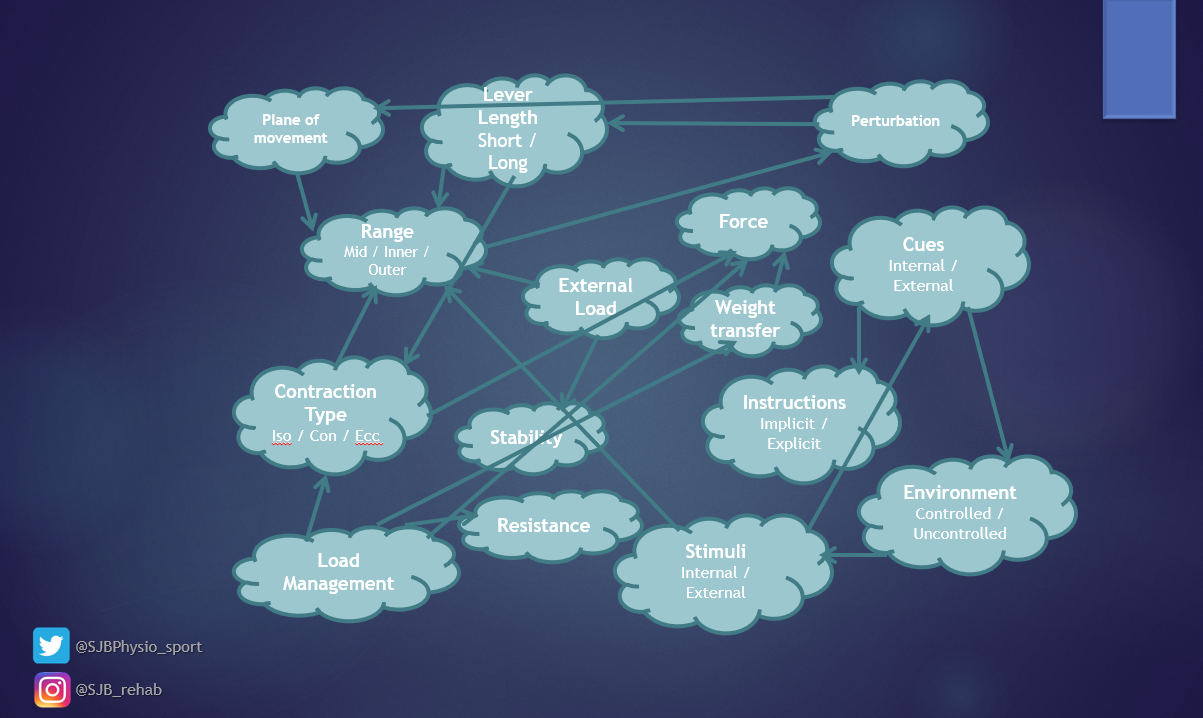
There are numerous variables that can be manipulated in a rehabilitation program in order to place appropriate levels of stress on the recovering patient/athlete. In my Masterclass on Clinical Reasoning in Rehab, I spend one module talking about many of these variables. With so many variables to choose from, I talked in depth about contraction types, cues, stability, and planes of motion.
In this blog I wanted the opportunity to discuss another variable – range of movement. Like the other variables, range of movement is intertwined and connected to so many others in a web of options we can tweak, progress and regress in the presence of injury.
Taken from my Masterclass on Clinical Reasoning in Rehab
Range of movement is a physical attribute that we assess as part of an acute injury, for clearance from injury to return to sport, and as an objective measure for each stage in between that. We look at it to monitor healthy joints or assess limitations as part of mitigating risk. It is something that needs to be considered with every exercise prescription, progression and regression. For these reasons, let’s look a bit further into how and why “range” is so important.
Length Tension Curve
One contributor to range is muscle length and to understand how we can influence this, we have the ‘Length-Tension curve’. On the curve we have three key zones, the inner range, the resting length, and the outer range.
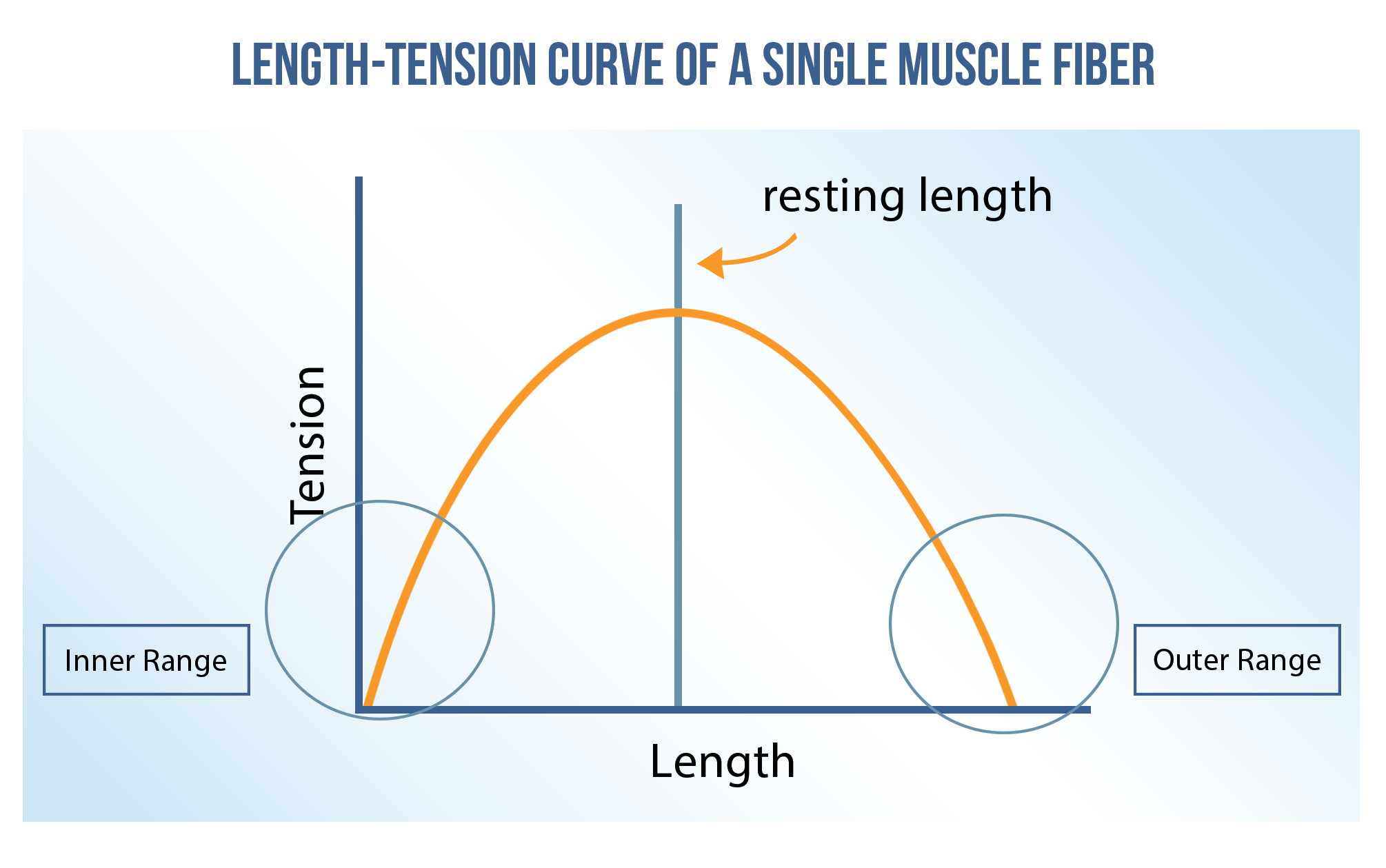
For this, let’s consider the interaction of thick and thin filaments in a sarcomere. In particular the myosin cross-bridge formation with actin. With a sarcomere in its most inner range, the cross-bridge formations are fully formed and there is little to no room for any further contraction. In this range we aren’t going to produce any force, if anything we are probably going to cause a cramp.
Alternatively, at the other end of the curve we have the outer range, this may be where we have one or two myosin heads in cross-bridge formation, but the sarcomere is going to be largely inefficient as it has a long way to contract before it can produce any real force. When we get beyond a point where a meaningful active contraction can occur, we have increased the passive tension on a muscle.
A good example here is the use of PNF contraction, where we get a small contraction before attempting to change the passive length of a muscle. We should be mindful in these ranges that people are weaker for this reason – they just can’t produce the same force.
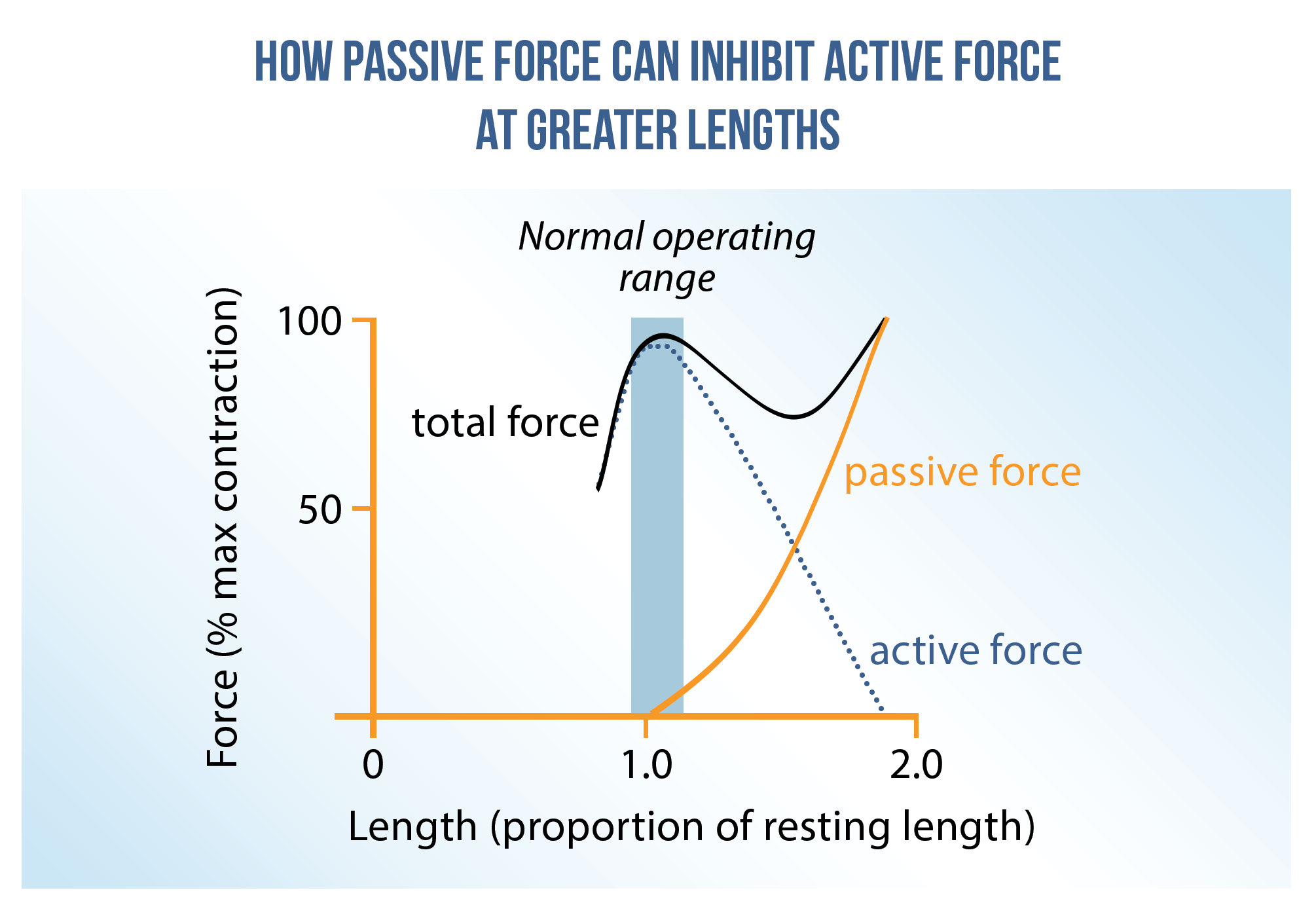
It is in the mid-range that we are most efficient, due to a good number of cross-bridge formations but with enough room either way to contract (concentric) or lengthen (eccentric). The body is very clever with this – our resting length for sarcomeres is in this mid-range position, so we can quickly and effectively tense a muscle. From a rehab point of view, if we are looking to increase muscle / sarcomere length, we need to ensure we get people strong in those ranges too.
Let’s look at a working example for context
Biceps femoris has its greatest maximal voluntary contraction into flexion, working as an agonist, at 0 and 45 degrees. It is weakest at 90 degrees (1); remember what we said about that inner range and the sarcomeres having nowhere else to go with their contraction? The resting length of the fascicles is at 40 degrees, so it is most primed for maximum contraction in this range. Don’t be confused, the resting length of the fascicles is not always a neutral joint position – it’s the point where the body thinks “this is where I need to be strong, quickly”.
Joint Space
Range of movement is not only affected by active structures, but is also heavily influenced by passive structures like bone, ligament and joint capsule. A good example is the hip – a mobile ball & socket joint, hip range movement is thought to be dependent on femoral version (ante or retro), femoral head angle (alpha angle), acetabulum coverage (shallow or deep), and the presence of a cam deformity (excessive rounding of the femoral head) (2). Ultimately, decreased femoral anteversion, greater acetabular coverage and a cam lesion will significantly decrease hip internal rotation range (2).
All of these are things that we as non-surgical clinicians are unable to influence, but knowing this might save you time and the athlete considerable discomfort by not hammering internal rotation range with very little gains. Instead with these cases, working on total hip range (hip flexion, pelvic tilt, external rotation) might be more beneficial.

Like with all MSK pathologies, previous injury is the biggest predictor of injury and pain. A study by Tak into hip injuries in soccer demonstrated that returning to sport after injury with reduced hip range significantly increased the chance of future problems (3). This study found that this was irrespective of the presence of a cam deformity, suggesting that morphology is one thing but restoring range where possible is within our capabilities.
Linking both joint space and muscle length, we have to consider when pathology affects stability vs rigidity. In 2015, I wrote a reflective piece exploring the mid-season management of a hip labral tear (4). This is a great example of compensation in the body where increased translation of the femoroacetabular joint is met by rigidity and fixation through the surrounding musculature (5,6). Typically, adductors and iliopsoas will attempt to increase congruency in the joint and therefore present as “tight” and with reduced range. The misconception here is that they are “too strong”, when in fact it is more likely they are providing the stability in the absence of control somewhere else.
Consider the demands of the sport. Don’t just fall into the trap of working through what I’d call the “action man ranges” – true anatomical flexion, extension, abduction and adduction. Watch training and competition of nearly all sports and you’ll rarely see these isolated sagittal or coronal movements. They tend to be combinations accompanied by transverse movements of the body in relation to the limb. Make sure this is replicated in your rehab.
Planes of Motion
Whether you consider it a plane or a range, you should start with contraction in a neutral position for acute injuries. This allows you to progress through unaffected planes, then the affected plane before increasing the complexity of movement to multi-planar exercises.
Let’s use a hamstring strain as an example and introduce a concept I term “contraplanar”.
If we know what plane of movement a tissue was injured in, typically for hamstrings it would be a sprint or stretch through the sagittal plane, contraplanar exercises could be employed early on to work the hamstring synergistically. For example, an adductor bridge, hip abduction, or this exercise below – single leg balance with upper body rotation.
In this exercise the hamstring is working at a low level to control the femur about a fixed pelvis and knee, working against transverse rotation which is occurring in the trunk, but not lengthening through any range in the sagittal plane. Therefore, contraplanar exercises may offer a good opportunity to optimally load in the early stages.
The single leg balance exercise presents a good example of progressing through the transverse plane. It offers sagittal plane stability in the lower limb and mobility through the transverse plane in the trunk. We term this dissociation and it’s quite complex to perform but the process is cyclical. Working against range for stability and then through range for controlled mobility.
In my Masterclass on Clinical Reasoning in Rehab, I give other examples of this multiple plane approach.
Conclusion
In this blog we have looked at different ends of the spectrum, from inner to outer range, considering acute injury and requirements for return to sport. Hopefully some of the discussion here has given you food for thought on how to apply this to many different types of injuries and locations, and made you think about your rehab prescription a little further. This is by no means an extensive list and I love learning about new ideas and concepts so please feel free to share your ideas and interpretations.
Want to learn more from Sam Blanchard?
He has done a Masterclass lecture series for us on:
“Clinical Reasoning in Rehab”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!