How to Prescribe Upper Limb Plyometrics

This blog is a follow-on from my previous blogs on A Physio’s Guide to Plyometrics (1) and The Rehab Continuum (2). These blogs outlined general exercise prescription guidelines and then drilled down into the nitty gritty of plyometrics. However, most of the content used examples from the lower limb and I found myself feilding lots of questions around how this relates to upper limb rehabilitation and performance.
Again, I would like to give a tip of the cap to the great masterclasses Physio Network has here that I completed and really solidified my thoughts around these topics; Exercise Prescription in Sports Rehab by Dr Teddy Wilsey, and Clinical Reasoning in Rehab by Sam Blanchard. (3,4)
So here goes – the clinician’s guide to upper limb plyometric prescription! Firstly, let’s not re-invent the wheel. The same phased continuum of increasing biomechanical demands applies as it did to the lower limb. There are however key considerations between upper and lower limb biomechanics that affect plyometric prescription.
Key Differences Between Upper and Lower Limb Plyometrics
- There is no set “athletic position” or “athletic movement pattern” for the upper limb that is uniformly applicable to most tasks / sports. This means that the position that we need to develop plyometric capacities in will be highly individualised throughout the multiple planes the upper limb can move based on injury loading characteristics and sporting / life demands (5).
- Plyometrics for the upper limb can be isolated to target a specific musculotendinous unit (more useful in early phase), or integrated into a whole kinetic chain to facilitate more functional movement / activation patterns (more useful in early and late phases) (5-7).
- The upper limb is more often challenged with rapid open chain plyometric functions in sports (throwing, striking) as opposed to closed chain. This should be considered in late stage rehabilitation (5).
- The extremely high rotational speeds (7000-9000 degrees per second) of upper limb sporting demands means tolerance to high deceleration impulses often needs to be built (think throwing a baseball vs jumping). This should be considered with end stage rehabilitation (5,8).
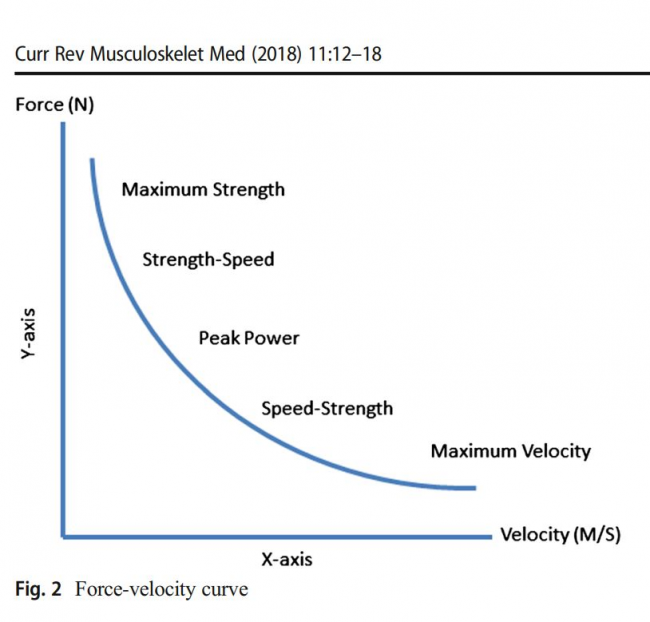
- For this reason, ensuring you have “surfed the force-velocity curve” in upper limb resistance training rehab is vital alongside your plyometric continuum. See Figure below (8).
For rehabilitation purposes it is generally recommended to perform a mixed / concurrent programming approach containing both plyometric and traditional resistance training exercises as opposed to plyometric exercises alone (8). Programs should include 2-5 sets of 1-6 contacts per set, 2-3 times per week, with a minimum 48 hours between sessions.
The use of upper limb plyometrics in rehabilitation only rates as evidence level D in clinical trials, however is strongly supported by expert opinion, with commonly prescribed upper limb plyometric exercises often far exceeding commonly researched movements in sports specificity and intensity (9). Therefore the evidence based recommendation of limited clinical utility with upper limb plyometrics should be called into question, as research hasn’t often matched clinical practice.
Upper Limb Plyometric Continuum
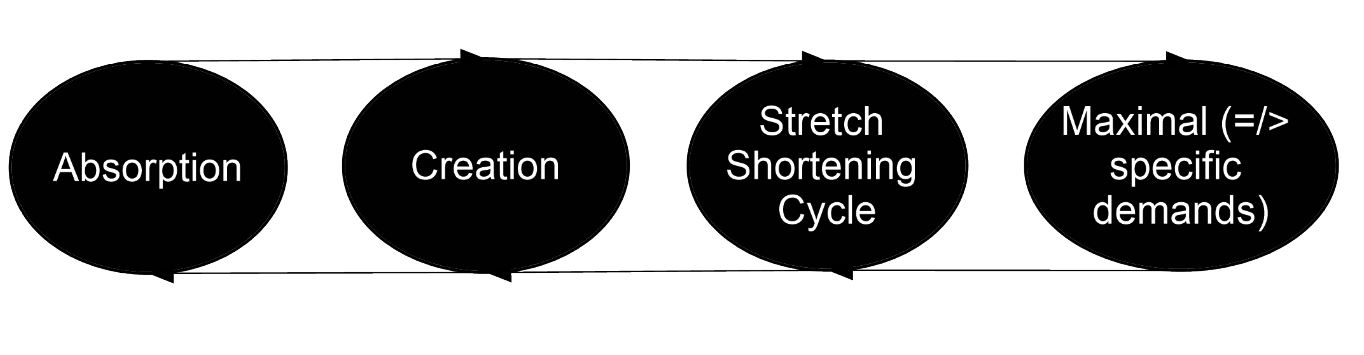
Force Absorption Phase
Remember the same rules apply here to beginning an upper limb plyometric program as they do a lower limb one. Refer back to my blog – A Physio’s Guide to Plyometrics.
A really thorough assessment of the function of the force absorption phase in your upper limb plyometric is important here. Which tissues are you needing to increase force absorption capacity in? How is it those tissues will be used in the goal movement?
For example, throwing a ball / tennis serve begins with an initial slower stretch shortening cycle through the anterior shoulder girdle muscles (predominantly pectoralis major), then finishes with a rapid stretch shortening cycle through the posterior shoulder girdle (primarily the posterior cuff muscles). This may mean returning a thrower or tennis player to plyometrics will consist of progressing either the anterior or posterior shoulder through force absorption (or even both) depending on injury. The goal speed of force absorption may differ drastically as well.
This phase consists of very basic exercises:
- Catching body weight in closed chain
- Catching a ball / weight in open chain with a plane or pattern you decide is needed.
- Med ball catch, particularly for reconditioning tissues post any form of biceps brachii or SLAP related issue.
Force Creation Phase
In this phase and the previous we can use the plinth to block isolated internal and external rotation throws and catches as well, as per the exercises of Maenhout et al (6). Clinically however I have found only very limited utility in these commonly researched movements.
My favorite test to use here, also doubles as an exercise – The single arm med ball put. We want to be aiming for around 70-75% Limb Symmetry Index (LSI) in this phase.
This phase consists of the following types of exercises:
- Single clap push ups
- Pendlay rows
- Bench throws
- High pulls
- Ball throws for distance (med ball or sports specific balls / implements).
Stretch-Shortening Cycle Phase
Now we can put reps of the previous movement together in quick succession.
The assessments we have previously performed should be close to 90% LSI.
Here I will also almost always have tested a shoulder hop test to get an idea of upper limb plyometric capacity.
The key thing to remember here is that it’s not only load that increases the forces on the musculotendinous unit, so does the speed of the amortization phase. So we need to begin to bump this up with intent to move quickly.
This phase consists of the following types of exercises:
- Plyometric push ups
- Push press
- Wall balls
- Med ball catch and throws
- Banded open chain position specific wobbles
- Repeated banded striking
Maximal Demands Phase
By this phase we should have surfed the force-velocity continuum and the upper limb should be ready to be involved in really high velocity tasks again.
All previous assessments should be greater than 95% LSI and we should be testing competence in goal-specific tasks.
This phase consists of the following types of exercises:
- Shoulder hops
- Push jerks
- Reactive cuff catches
- Specific banded wobbles
- Return to sport specific throwing
- Hitting / striking training
Conclusion
So there we have it, the plyometric continuum as you may not have seen it before – used for the upper limb. The main point to remember when rehabbing an upper limb sports injury is that, as physiotherapists, we still need to have the same checks and balances of all the components of the musculotendinous units’ ability to transmit force as we did in the lower limb. So just be thorough, be methodical, and you’ll be fine!
Want to learn more about shoulder injuries?
Rod Whiteley has done a Masterclass lecture series for us on:
“The sporting shoulder”
You can watch it now with our 7-day free trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!