Ankle sprain solutions: An expert physiotherapist’s strategies for success

Poor management of ankle sprains can lead to the development of chronic ankle instability. Pro tips from leading physiotherapist David Hillard can help you to master your management of ankle sprains, and ultimately achieve the best outcomes for your patients. In this blog, we’ll outline David Hillard’s Practical on managing ankle sprains.
The interventions we’ll cover include:
- Manual therapy
- Taping techniques and shoe inserts
- Exercise progressions
If you want to see exactly how expert physio David Hillard manages ankle sprains, watch his full Practical HERE.
Manual techniques
Manual therapy techniques can help improve Range Of Motion (ROM) and decrease pain to enable your patient to participate in rehab exercises more freely. These hands-on techniques are more likely to be helpful for acute and/or painful ankle injuries. The primary approaches are soft tissue mobilisation for swelling reduction, and joint mobilisations to improve ROM and reduce pain.
In the below video taken from his Practical, David demonstrates a technique for soft tissue release and joint mobilisation:
Taping and Shoe Inserts
In addition to manual therapy, we can also improve tolerance to loading through the use of taping and shoe inserts. Taping in acute ankle sprains is an excellent stopgap tool to offload painful areas and improve weight bearing. In addition to traditional taping techniques which stabilise the ankle, taping can address issues such as posterior ankle impingement, as David shows us in this snippet taken from his Practical:
For shoe inserts, there are several options available. A heel wedge keeps the ankle in plantarflexion, which can be helpful for injuries such as a high ankle sprain in which weight bearing dorsiflexion causes pain. Another option is obtaining prefabricated orthotics for injuries where increased medial arch support is needed, such as deltoid ligament sprain.
Exercise Progressions
Now we’ve covered the ‘external’ aids of manual therapy, taping, and shoe inserts, let’s dig into the crux of our management plan – exercise.
Foot and ankle exercises
Early on, the priority is to regain ROM and redevelop ankle and foot intrinsic muscle strength. Typically, we prioritise improving dorsiflexion ROM, since this crucial motion often becomes limited post-sprain. There are many options to address this, such as Mobilisation With Movement (MWM), where a posterior talocrural glide is applied as the patient moves through dorsiflexion. Training foot intrinsic muscles is especially important for patients who have been immobilised in a boot and/or non-weight bearing.
Ankle strengthening largely targets the muscles of dorsiflexion, inversion, eversion, and plantarflexion. David uses an exercise which loads the peroneal muscles while simultaneously strengthening the glutes (which often weaken in patients with chronic ankle instability), he demonstrates this in the below video taken from his Practical:
Initial plantar flexion training usually involves bodyweight heel raises, however, most athletes will need external loading to develop sufficient calf strength to return to sport. We want to include loading that biases the soleus and the gastrocnemius (i.e. flexed knee and extended knee heel raises).
Balance training
This should include both static and dynamic balance exercises. A key note on balance training is that the ankle should eventually be challenged at end ranges (e.g. in plantarflexion), instead of only training balance with the foot flat on the ground.
Static balance training can be progressed in a variety of ways, including using compliant surfaces, closing the eyes, adding external loads or rotating the body to change the athlete’s centre of mass, altering contact of the foot with the ground, and adding reactive demands such as throwing/catching. For example, starting with single leg stance – this can be progressed by using a compliant surface, then balance could be challenged further by adding a multidirectional throwing/catching task.
Dynamic balance training can also be progressed in similar ways (i.e. using compliant surfaces, adding external loads, altering contact of the foot with the ground, rotating the body). As an example, you could start with tandem walking, then progress to tandem walking on the toes, and then add head turns.
Multi-joint strength training
In addition to redeveloping balance, the athlete needs to rebuild strength in foundational movement patterns. Multi-joint strength training refers to larger, compound movements which involve the whole lower extremity. To start, we have standard strength and conditioning exercises like lunges, squats, and deadlifts (the unilateral variations being especially useful post ankle sprain). Athletes should also perform exercises which retrain locomotive patterns, as David demonstrates in this snippet taken from his Practical:
When the athlete demonstrates sufficient strength and endurance (those needs will vary based on their unique circumstances) and tolerance to loading, we can start to introduce them to rapid loading with plyometrics and running.
Plyometrics and return to running
Plyometric training varies widely as it’s influenced by factors such as the severity of injury and type of sport/activity. For example, after a grade one lateral ankle sprain, an athlete may only need to check off a few running drills before returning to running, whereas after a grade three sprain with fracture, running drills may need to be practiced several times before jogging.
With plyometrics, the least intense/complex exercises are: low amplitude (i.e. low height and/or horizontal distance), bilateral, concentric focused (minimal eccentric landing loads), single repetition, performed on compliant surfaces with rebound, and/or uni-directional (e.g. vertical pogo hops). The chart below shows this beginning tier and what progressions look like for each variable:
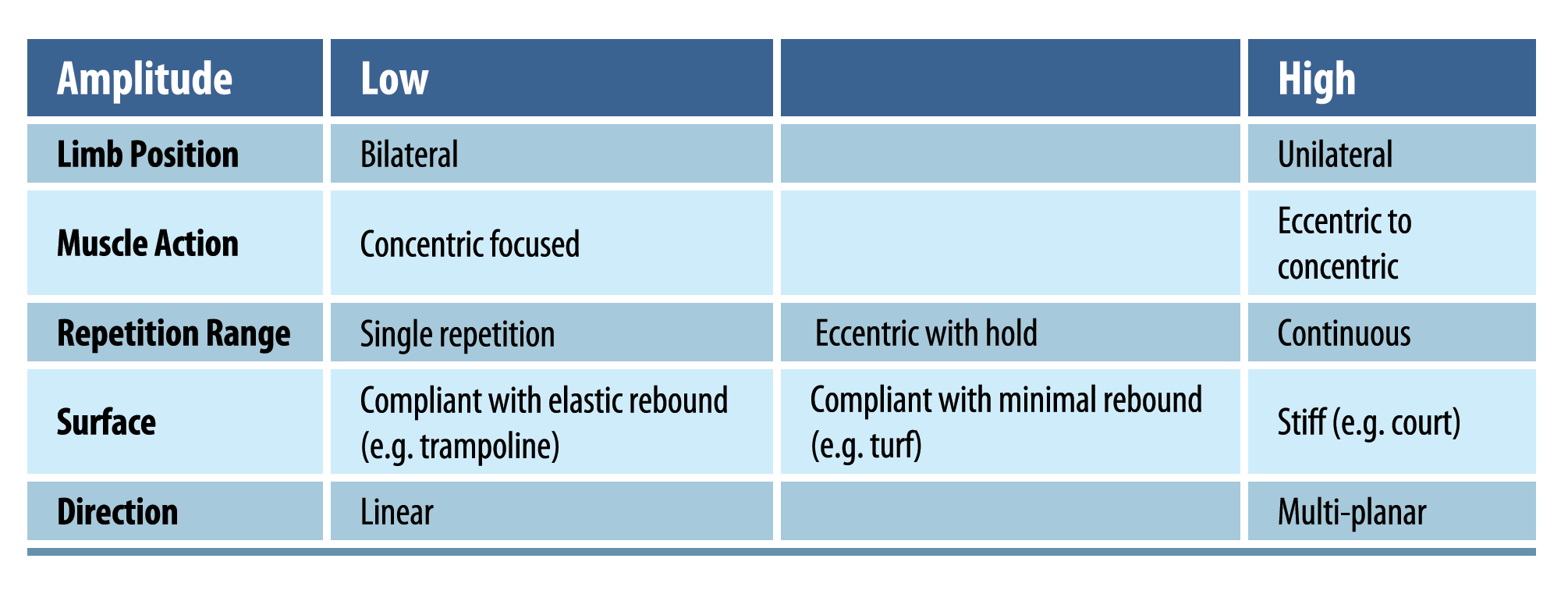
Rather than a cookie-cutter approach to plyometric training, think in terms of manipulating certain variables to progress in a way which is relevant to the athlete. This gives you much more flexibility and helps you troubleshoot when an athlete runs into a problem in their rehab.
Acceleration/deceleration, and change of direction
As the athlete successfully progresses through plyometric training, we can start to introduce more sport specific work including acceleration, deceleration, and change of direction. These drills not only develop the necessary ankle stability to return to sport, but also help restore the athlete’s confidence in their ability to perform. Drills can be progressed by modifying variables such as direction of movement, the time and/or space for performing the change in movement (e.g. decelerating over a limited distance), the angle of the turn (e.g. a 45-degree turn is less demanding than a 90-degree turn), and adding reactive demands such as shadow drills.
For example, an athlete could start with a shuttle run, then progress to a C-curve run, and finally to zig-zag drills.
Wrapping Up
Optimal management of ankle sprains is crucial to get athletes back to play and reduce the risk of long-term ankle instability. It may also be important to consider how to keep the athlete training during rehab to maintain fitness and confidence. Mastering your management of ankle sprains takes time, but this blog provides you a solid framework, and outlines the many tools at your disposal to get the best outcomes for your patients!
For a comprehensive understanding on how the experts manage ankle sprains, be sure to check out David Hillard’s Practical HERE.
👩⚕️ Want an easier way to develop your assessment & treatment skills?
🙌 Our Practical video sessions are the perfect solution!
🎥 They allow you to see exactly how top experts assess and treat specific conditions.
💪 So you can become a better clinician, faster.

Don’t forget to share this blog!
Leave a comment (1)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
For patients whose injury occurred over 6 months ago, but are still struggling with pain and swelling, what is the best way to handle this in case of optimal load, repetitions, sets, and pain and what guidelines can I give my patients regarding sports activities: how often, how much, how long, or how much to restrict?
Kind Regards Valentina