
Background
Hip pain is complicated, with many possible and sometimes overlapping sources of pain making diagnosis a challenge (1,2). Younger adults (aged 18-50 years) may have had hip pain for months or years at the time of assessment (3), making it even more difficult for clinicians to know where to start. This blog will provide a guide for physiotherapists to perform an evidence-based assessment for the diagnosis of the source of hip pain in younger adults.
For a more in-depth look at how to practically assess hip pain, be sure to check out Jo’s excellent Practical – where you can watch a 1 hour video recording showing exactly how she assesses the hip.
Three recent consensus agreements have provided clear advice on how to classify hip or groin pain. These provide clinicians with a simple framework that can be used to guide the assessment process. The Doha agreement (1) described five non-red flag clinical entities causing groin pain:
- Adductor-related
- Pubic-related
- Hip flexor-related
- Inguinal-related
- Hip-related
The Zurich agreement (2) then described hip-related pain as having three likely sources: 1. Femoroacetabular Impingement (FAI) Syndrome; 2. Acetabular dysplasia/hip instability; and 3. Other sources of pain without abnormal bony shape (e.g. cartilage or labral tears). The Warwick agreement on FAI syndrome stated that a diagnosis of FAI syndrome required the presence of symptoms, signs and positive imaging findings.
This blog was developed using two excellent resources (4,5), but does not discuss the use of imaging (due to word limits). However, there are a number of recent publications that provide an excellent overview of imaging and hip pain (2,6,7).
The evidence-based assessment consists of four parts:
Part 1: Subjective Assessment
The following is not an exhaustive assessment, but will give the clinician some guidance about key components specific to younger adults presenting with hip and groin pain:
- Age is important, as the male pelvis is not skeletally mature until often after 25 years of age, meaning pelvic apophysitis is common in younger men. Hip osteoarthritis also needs to be considered in people aged over 35 years.
- The type of sport played should be discussed, as kicking sports and those involving direction change commonly cause hip and adductor or pubic related pain; while long distance running, gymnastics and dance can be associated with stress fractures.
- Load management is also important, especially for recurrent injuries, or when bony stress injuries are possible.
- Teenage sporting history during years of rapid growth can provide insight into the likelihood of cam-type FAI syndrome, as the development of cam morphology is associated with high loads especially in rotation during these years.
- A strong family history of hip pain is associated with increased risk of cam morphology and also possible hip osteoarthritis.
- Hip injury or pain during childhood can suggest a history of hip dysplasia or slipped upper femoral epiphysis and should be explored.
- Pain at rest and at night could indicate synovitis (inflammation within the hip joint) which is commonly seen in patients at hip arthroscopy.
- Reduced capacity to sit for long periods of time is seen commonly in FAI syndrome and hip osteoarthritis.
- The presence of mechanical symptoms with pain such as clicking, locking, catching, and giving way can suggest labral injuries.
- Pain on twisting, especially if onset is sudden, can indicate labral, cartilage or ligamentum teres injuries.
- Pain location can greatly assist in diagnosing the clinical entity involved.
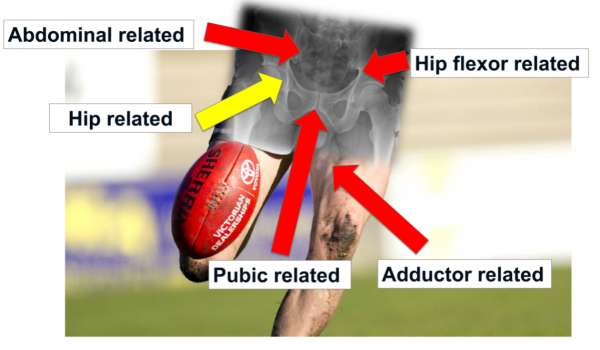
Pain location and possible sources of pain, based on the Doha agreement of clinical entities (1)
Learn more about how location of pain can help inform your diagnosis in this snippet from Jo’s Practical.
Part 2: Screening for Red Flags
Red flag screening is critical for people with hip pain. Be aware of:
- History of cancer – as prostate, breast, gynaecological cancers can all metastasise to the hip.
- In women, gynaecological causes of pain can be experienced in the hip and groin region, so always ask about menstrual cycle and history of gynaecological issues.
- Unexplained weight loss may indicate cancer.
- Burning with urination can suggest urinary tract infections.
- Change in bowel habits can indicate bowel cancer or other bowel disease.
- Alcohol abuse can predispose people to avascular necrosis (AVN).
- Corticosteroid exposure can expose people to AVN and stress fractures.
- Acute pain with fever can indicate intra-articular infection.
Part 3: Ruling out the Lumbar Spine and Pelvis
The lumbar spine and pelvis can often refer pain to the hip and groin region. The following signs can assist in ruling in or ruling out the lumbar spine and pelvis as a source of pain:
- Walking with a limp suggests the pain is seven times more likely to be related to the hip than spine.
- Pain in the groin/anterior hip suggests the pain is seven times more likely to be related to the hip than spine.
- Reduced hip IR ROM suggests the pain is 14 times more likely to be related to the hip than spine.
- No change in symptoms with repeated lumbar movement has a sensitivity of 92% to rule out the lumbar spine as a source of pain.
- Negative extension/rotation of the lumbar spine has a sensitivity of 100% to rule out the lumbar spine.
- Negative straight leg raise (SLR) has a sensitivity of 97% for ruling out the lumbar spine.
- Negative slump test has a sensitivity of 87% for ruling out the lumbar spine.
Part 4: Using the Objective Assessment to Aid Diagnosis
Components of an objective assessment and imaging can aid the physiotherapist in coming to a diagnosis, but cannot do so in isolation. The two components of the objective examination that assist most with diagnosis are palpation and diagnostic (special) tests.
Palpation
- Similarly to pain location, palpation of the potentially implicated structures can aid in diagnosis. Palpation can help determine whether symptoms are adductor-related, pubic-related, inguinal-related, or iliopsoas-related.
Diagnostic tests (special tests)
- Most diagnostic tests assist in ruling out a specific diagnosis (most tests have a high sensitivity, meaning it is unlikely to get false negatives) than ruling in a condition (most tests have poor specificity, meaning it is very likely to get false positives).
- The Flexion-Adduction-Internal Rotation test (FADIR) test has high sensitivity (94-99%) and low specificity (5-25%) (2,4,8). This means that a negative FADIR test should be used only to rule out the hip joint as a possible source of pain (note – a negative test means that the test does NOT reproduce the patient’s familiar pain). A positive test does not assist in diagnosis.
- Similarly, the Flexion-Internal rotation overpressure test (internal rotation overpressure at 90° flexion) has a high sensitivity (70-98%) and low specificity (8-43%) (2,4,8). This test should be used in the same way as the FADIR test, where a negative test can assist in confirming the hip as not being the source of pain.
- The commonly used Flexion-Abduction-External Rotation (FABER) test has poor sensitivity and specificity, and therefore should not be used to diagnose the source of hip pain.
- The adductor squeeze test has high specificity (91%) and poor sensitivity (43%), meaning that a positive test can aid in confirming the presence of adductor-related groin pain.
- The ligamentum teres test is another special test for hip pain. Learn how to perform it and what a positive and negative test means in the video below, taken from Jo’s Practical.
Hopefully this blog has provided you with some useful insights into how to differentially diagnose hip pain in young adults, allowing you to be more confident and accurate in your clinical assessment.
To learn a whole lot more about how to practically assess hip pain, be sure to check out Jo’s fantastic Practical.
👩⚕️ Want an easier way to develop your assessment & treatment skills?
🙌 Our Practical video sessions are the perfect solution!
🎥 They allow you to see exactly how top experts assess and treat specific conditions.
💪 So you can become a better clinician, faster.

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!