Treating Adductor Related Groin Pain. Not just a pain in the hip!

Groin pain is a common clinical entity faced by clinicians, particularly those who treat athletes. To complicate matters, distinguishing adductor related groin pain (ARGP) from other differential diagnoses can be challenging as multiple structures coexist around the anterior pelvis. Clinical features include (16):
- Pain on palpation of the adductor tendons
- Reproduction of symptoms with adductor contraction
- Pain with passive stretching
The prevalence of groin injury is approximately 13% and 7% in men and women respectively, especially in those with strength deficits (19). Furthermore, those with previous injury are 2-4x more likely to develop a recurrence so it is imperative that rehabilitation is progressive and exposes the musculature towards the stressors associated with their sport. For further information around ARGP, check out this Masterclass by Dr. Andrea Mosler on groin pain in athletes.
When looking to rehab the adductor musculature, we must consider the multiple functions they have upon the movement and stability of the hip and include this in our exercise programme.
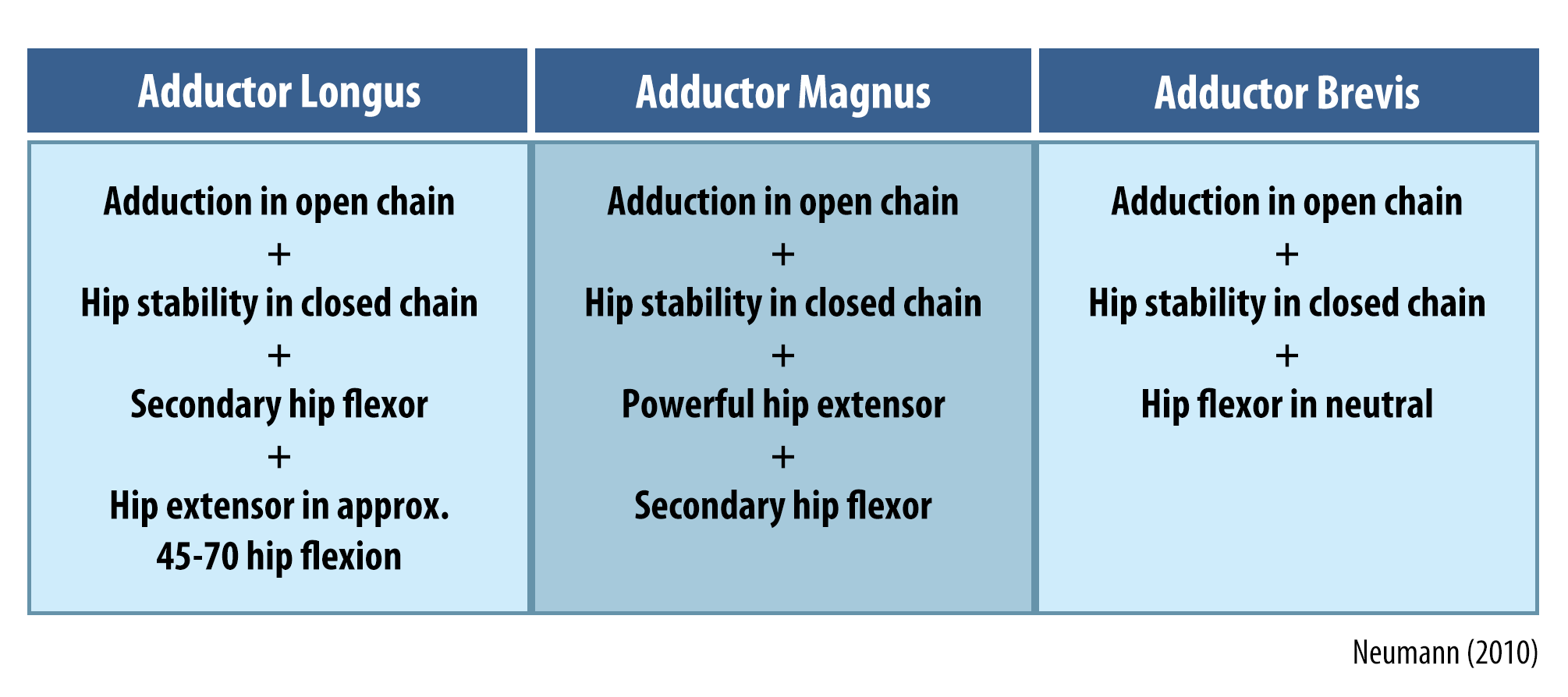
Triplanar demand is placed through the adductors which may explain why injuries account for around 69% of groin pain. In particular, adductor longus is most susceptible due to a lack of mechanical advantage coupled with a small insertion and reduced vascularity which is likely to slow down recovery following microtrauma (13).
Training considerations
Rehabilitating injuries is likely to follow more of a linear periodisation programme, especially during the initial to intermediate stages as the capacity of the musculotendinous unit will not be able to withstand more advanced and higher intensity training.
Periodised programming has consistently been found to elicit greater adaptations in muscular strength and hypertrophy because of the following benefits (5):
- Progressive, neuromuscular overload
- Managing fatigue
- Preventing plateau
Following the initial phase of acute injury management, focus should turn towards progressively loading the adductors and surrounding muscles with the aim of improving strength asymmetries. This is vital because ADD/ABD strength ratio of <80% is thought to predispose athletes to a 17x greater risk of groin injury (5). More recently, a modified rehabilitation programme focusing on; a) intersegmental control, b) linear running mechanics and load tolerance and c) multidirectional movements coupled with high-speed sprinting has led to faster return to play (RTP), averaging around 9-10 weeks (8, 1).
Isometrics
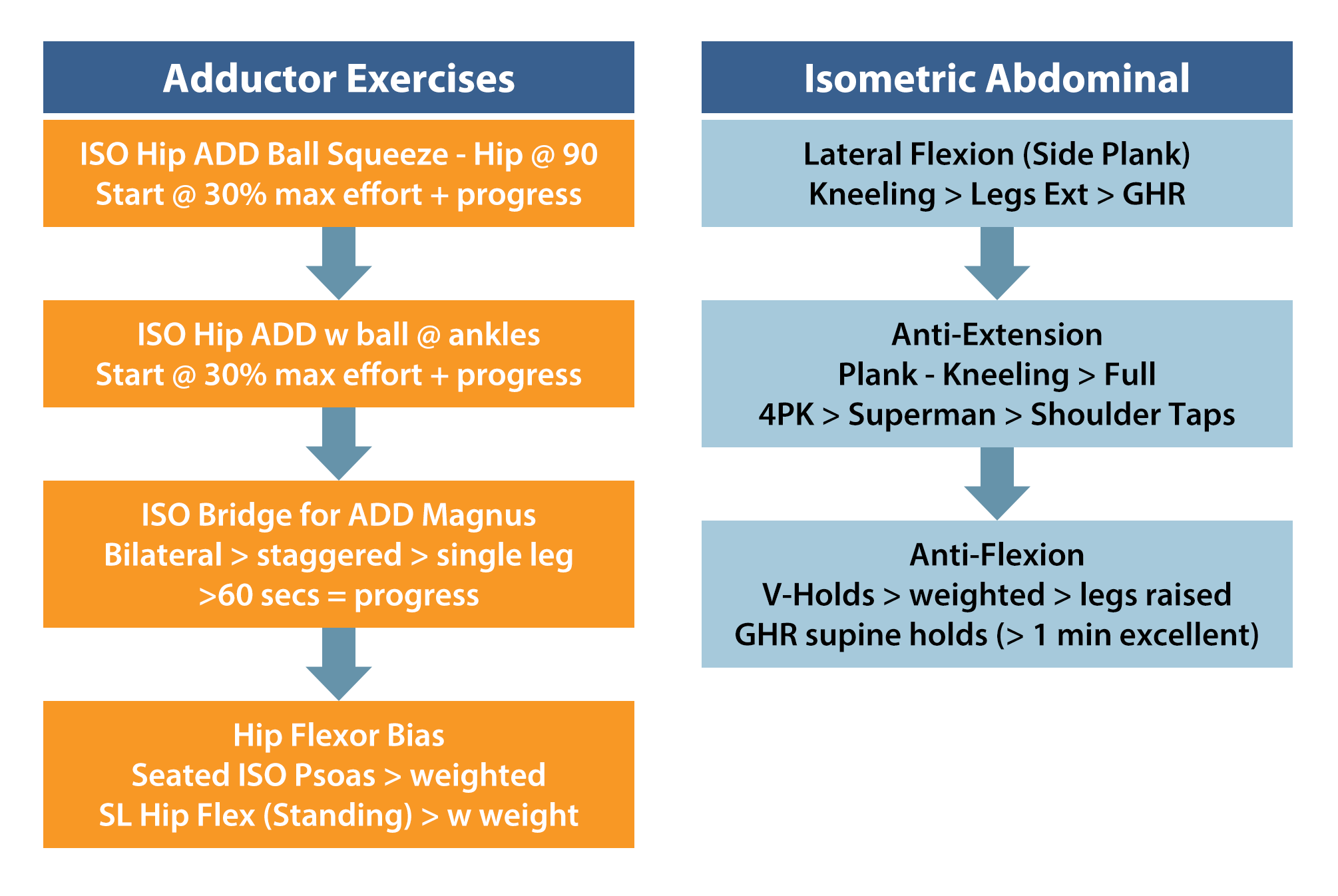
Isometrics are often a staple in most programmes and appear to be efficacious in the treatment of ARGP. For example, in field sports the adductors will have to isometrically contract on the stance leg during kicking to stabilise the pelvis. Three exercises with EMG’s >60% which are thought to elicit strength gains are (13):
- Isometric hip adduction – ball between knees (108%)
- Isometric hip adduction – ball between ankles (86%)
- Copenhagens (108%)
Some additional isometric exercise examples can be found below;
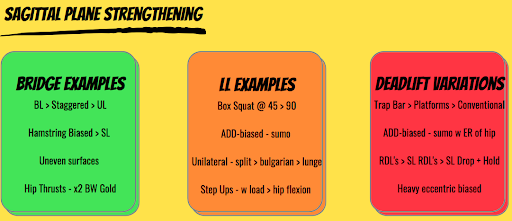
Sagittal plane loading of the adductors is another training method which is emphasised during the earlier stages of rehabilitation as this is considered less provocative than frontal plane exercises (7).
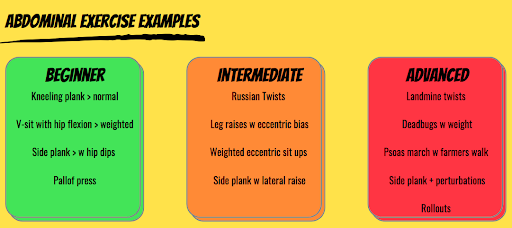
Abdominal exercises
The abdominals work antagonistically to the adductors during movements such as kicking whereby they have to eccentrically oppose movement of the leg to help maintain pelvic stability. Research has found that footballers may have reduced eccentric abdominal strength which can compromise pelvic stability, imparting greater load through the pubic symphysis and adductor musculature which may increase the risk of injury (10, 15).
Below are some examples. These can be added as accessories to a workout, performed in isolation or I quite like to implement 2-3 prior to workout / training session as part of a warm-up.
Frontal plane exercises
Following a period of sagittal loading coupled with symptoms settling, frontal plane exercises can be integrated into the programme and are integral as a large percentage of injuries will occur during eccentric loading of the adductors within this plane (i.e. rapid hip abduction, kicking and change of direction). Examples include:
- Lateral step ups
- Lateral step downs
- Lateral lunge (98%)
- Open chain adduction – banded / cable-pulley (103%)
Serner et al., (2013)
Objective measurements
Patients should possess an adequate amount of muscular strength, particularly under eccentric load in order to tolerate plyometric and ballistic-based exercises which utilise stretch-shortening-cycle (SSC) and reactive strength (9). The following principles should be applied to encourage this:
- Loads of >80% 1RM to promote neural drive and motor unit recruitment
- Mid-high weekly set ranges, no more than 15 per muscle (12, 6).
- No more than x2 sessions/week with at least 48 hours recovery.
Below are some anecdotal targets which athletes can aim towards as part of their strength training.
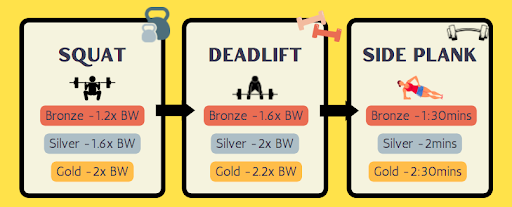
1.6x bodyweight in weightlifting derivatives is considered optimal before commencing power-based training as individuals with greater muscle strength possess better physiological attributes for improving power (9, 3).
Those with ARGP have reduced reactive strength with longer ground contact times vs uninjured athletes (1). Exposing athletes towards training modalities such as ballistic strengthening and plyometrics can improve rate of force development. This transfers to sporting activities and is a key component of rehabilitation which improves intermuscular coordination and neural drive which ensures athletes possess the physiological attributes before commencing sprinting and change of direction drills (4, 8).
Considerations for training power
- Lighter loads = faster velocities = more applicable to sporting scenarios
- Short + rapid contractions – 100-250mms for activities like sprinting and jumping
- Quality > quantity (avoid high volumes of training to minimise neuromuscular fatigue)
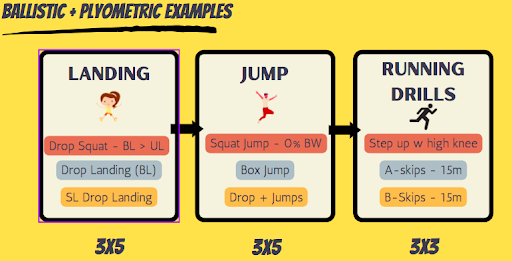
Other considerations from above
- Putting the brakes on (landing drills) – developing eccentric strength to attenuate load
- Progress from bilateral > unilateral > to greater heights
- Using the accelerator – maximum concentric contraction following eccentric loading to fully utilise SSC and promote gains in muscular power which correlate to sporting activity.
- Consider training these throughout all planes
- Progress from bilateral > unilateral.
Objective testing
- Triple hop test (measure distance)
- Countermovement jump (measure ground reaction forces)
- Lateral hop test (look at ground contact times)
Running
In terms of programming, this goes beyond the scope of this blog. I do, however, really like the work by King et al (2018) and Baida and colleagues (2021) which encourage a graded approach to running.
Athletes initially focus on a linear running programme which progressively builds in duration and speed. Once completed, they commence linear sprinting which starts at sub-maximal levels and progresses to maximal intensity. During this stage, the therapist may wish to consider an undulating periodisation programme whereby the volume and intensity of sessions are frequently changed in accordance to the players schedule.
An example of how this may look is:
- Day 1 – lower-limb strengthening session
- Day 2 – sub-maximal aerobic endurance session
- Day 3 – plyometrics with abdominal accessory work
- Day 4 – rest
Athletes are then encouraged to subjectively rate the intensity and symptom response of the session, those which are deemed ‘green’ is considered a marker for the athlete to progress.
Change of direction (COD)
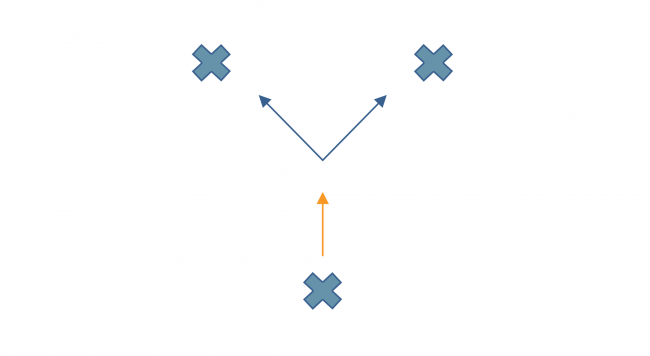
COD drills should focus on a variety of cutting manoeuvres with acceleration and deceleration which look to heavily load the adductor musculature in lengthened positions. The rationale is to progress the difficulty of each exercise so there is high physical demand placed upon the athlete accompanied by unexpected stimuli which would replicate a competitive scenario. Examples of this may include:
- Y-drill’s 3x10m with 2 minute rests:
- Spatial uncertainty, player sprints and has to cut last minute following instruction
- Universal uncertainty – involves opposition, player must react to unexpected stimulus
- Calculating volume in a session = sets x reps x distance (no more than 500m per session)
- 1:5-8 work rest ratio
- Same emphasis as plyometrics, taxing on the neuromuscular system so will require 48hrs between sessions.
Return to Play (RTP)
There will be significant variation regarding criteria which is dependent upon the sport. A Delphi survey agreed that assessment of strength, performance tests and sport-specific skills should support the RTP decision (18). This appears to be in agreement with Serner et al., (2020) who recommend three phases for effective RTP in football:
- Clinically pain free
- Controlled sports training
- Full team training which resulted in reduced reinjury rates compared to additional studies (14).
Strength
Calculate hip ADD/ABD ratio, >90% is considered appropriate for RTP whilst looking to minimise any strength asymmetries (15). Other examples of testing include:
Performance Tests
This will vary depending on the type of sport and amount of equipment available:
- T-test
- 40m timed sprint
- Illinois Agility Test – using a football for dribbling
- Countermovement jumps / lateral and forward hops (ground reaction forces + contact times)
Sport-Specific
For footballers, kicking imparts large compressive load through the adductor enthesis due to the eccentric loading during the wind-up motion followed by a powerful concentric contraction as the player strikes the ball. This is likely to become particularly challenging when performed under fatigue (2). Examples would include:
- Gentle passing > longer distance passing > maximal intensity shooting
- 1:1’s
- Jumping through all planes
- Shooting scenarios
Wrapping Up
I hope you’ve found this blog useful on treating ARGP. For more information, I highly recommend checking the Groin pain in athletes: unravelling the mystery Masterclass by Dr. Andrea Mosler’s
Want to learn more about the groin?
Dr Andrea Mosler has done a Masterclass lecture series for us on:
“Groin pain in Athletes: unraveling the mystery”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!