Update Your Management of Femoroacetabular Impingement with Dr. Jo Kemp

Femoroacetabular impingement (FAI) is a common lower extremity problem, especially in younger, athletic individuals. However, this condition can be quite painful and tricky to manage, so we sat down with hip expert Dr. Jo Kemp. Dr. Kemp is a physiotherapist, researcher, and educator who specializes in the non-surgical management of hip pain. These insights are from her appearance on our podcast Physio Explained, where you can learn from the best in 20 minutes or less. This talk focused on three keys to managing FAI: physiotherapy treatment duration, exercise dosage, and patient education.
How long does FAI rehab take?
A common issue in FAI rehab, is that we simply don’t give physiotherapy enough time. Research suggests that a patient needs at least 3 months to see significant improvement in symptoms (1). While there should be some improvement prior to the 3 month mark, patients need to know that significant improvements will take at least 3 months. Why might results take this long?
First, neuromuscular adaptations take time, so 6 week or shorter treatment plans are not long enough to reap the benefits of said adaptations. Second, as we physiotherapists know, some patients need more time to buy in and meaningfully engage in an exercise program. We can use the analogy of medication dosage to communicate the importance of a properly dosed exercise program.
For example, prednisone dose packs are often prescribed for 6 days. Much like this oral medication, exercise as an intervention needs to be “taken” at the prescribed dose and for a sufficient duration to see significant results. Our job as physiotherapists is to set these expectations, so that patients can give physical therapy a fair chance rather than rushing to invasive, expensive treatment options.

How do I dose exercise for FAI?
Traditionally, FAI rehab has focused on improving hip rotator strength and motor control. However, Dr. Kemp points out that active hip rotation in the patient with FAI can be quite irritating which may decrease adherence to an exercise program. Research has observed strength deficits in trunk and hip extension, adduction, and abduction (2,3,4). Interestingly, hip adduction strength in particular, is strongly associated with improvements in quality of life and thus an important target in FAI rehab (5). In terms of loading parameters, Dr. Kemp suggests developing strength endurance for the trunk and strength/hypertrophy for the hip musculature.
An example exercise program could be the following performed 2-3 times per week:
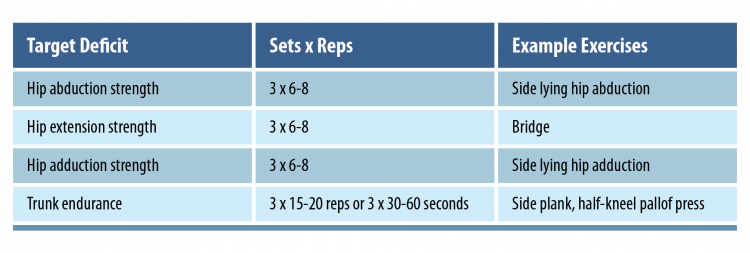
An important consideration when starting a program is that large ranges of motion may be uncomfortable, so starting with higher load exercises in a smaller range of motion may be better tolerated by many patients.
How do I educate patients rehabbing with FAI?
Dr. Kemp emphasizes the importance of education in patients with FAI. First, we need to educate patients that there is not always a clear correlation between the structural changes seen with FAI and pain (6). This means that while structural changes can play a role in their pain, we often can manage FAI through interventions that do not change the structure of the hip. This ties into educating patients that pain during exercise does not mean tissue damage is occurring, so it is acceptable to experience minor pain when progressing exercises (7).

Of course, we should make exercises relatively tolerable (otherwise we run into issues with adherence). But we need to reassure patients that experiencing minor pain during exercise is ok. Lastly, patients should know that flare-ups may occur and CAN be managed. In the short term, analgesics can aid in managing these flare-ups. For those patients concerned about excess medication use, we need to remind them that analgesics are intended for short term use.
Wrapping Up
FAI can be challenging to manage and may recur. Here are clinical pearls from this talk with Dr. Jo Kemp to help you better manage FAI:
- We typically need about 3 months of treatment to see significant changes
- Develop hip adduction, extension, and abduction strength with heavy loads (i.e. 3 sets of 6-8 reps)
- Develop trunk muscle strength-endurance (i.e. 3 sets of 15-20 reps or 3 sets of 30-60 seconds)
- Start with smaller range of motion exercises, then gradually increase, since large joint excursions can be painful
- Pain during exercise is OK, but should be minimal during and 24 hours after
🎙️ Learn from the best in 20 minutes or less
💡 Our podcast ‘Physio Explained’ takes you inside the minds of the brightest physios in the world.
🎧 You won’t find an easier way to learn on the go.

References
Don’t forget to share this blog!
Leave a comment (1)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
yep all makes sense; flexion ROM may also return; i do think you should work on hip flexor strength too . control of hip valgus whilst controversial should be examined