How to Dose Strength Training for Older Adults

With an aging population, we as physios see more and more older adults. However, a common issue is that we under-dose exercise, especially strength training. This issue has become so prevalent that the American Physical Therapy Association’s “Choosing Wisely” campaign recommends “Don’t prescribe under-dosed strength training programs for older adults” (1). In this article we’ll explore why proper dosage is important, why many physios under-dose, and how to properly dose strength training exercises. If program design for older adults is something you want to learn more about, check out Dr. Mariana Wingood’s masterclass here.

Why is proper dosage of strength training important?
With age, there is a loss in muscle strength and power, which can lead to decreased function and increased fall risk. It is estimated that after the 6th decade of life there is a 3.6% loss in muscle strength each year (2). Functionally, this means that older adults exert considerably more effort to perform daily tasks.
For example, research shows that to rise from a chair, a young person works at 42% relative effort while an older adult works at 80% relative effort (3). Thankfully, with strength training (and other forms of exercise like balance and cardiovascular training) we can increase that capacity so that older adults can function and live better.
If strength training is so important for older adults that begs the question…
Why don’t physios properly dose strength training for older adults?
Physios often don’t properly dose strength training because:
- We don’t want to cause injury to older adults
There is a valid concern regarding injury risk with older adults. Many older adults have complex medical histories, musculoskeletal pathologies like arthritis or osteoporosis, decreased tissue elasticity, and decreased recovery capacity. However, research shows that older adults can safely perform and benefit from strength training. For example, in a study where the average participant age was 90 years old, subjects performed strength training exercises at an intensity of 80% 1-Rep Max (% 1RM). The participants suffered no injuries and experienced strength gains of up to 174% from their baseline (4).
- We don’t want to risk causing adverse cardiac events with older adults
Any good physio doing a medical history will note that older adults tend to have more complex medical histories than younger ones. However, our expertise is designing programs specifically for complex patients. No matter the condition, your patient can exercise at a relatively high intensity. Monitoring of vital signs, patient symptoms and the use of scales like “Rating of Perceived Exertion” are crucial. For details on safe exercise parameters check out the Masterclass “Exercise Prescription in Aging Adults” by Dr. Mariana Wingood here.
- We believe that older adults don’t need to exercise intensely
We often assume high intensity exercise is the domain of young athletes, while older adults should be given “gentle” exercises. Unfortunately, this doesn’t help older adults perform activities of daily living or participate in hobbies or sports. As we discussed before, tasks like a sit to stand can become quite challenging so we need to sufficiently load our patients with exercise in order to function and live better. Our job is to educate them on the benefits of exercise and help them find a mode of exercise that fits their unique situation.

How to properly dose strength training
Here are three practical tools to dose strength training for your older clients:
1. Select a sufficient intensity for strengthening
To improve strength we need to train in the intensity range of 60-85% 1RM, with higher intensities resulting in greater strength gains. An intensity of 60% represents the minimum to get stronger, while the 70-85% range is optimal for strength adaptations (2).
Now, we can test % 1RM, however this can become quite time consuming when performing a variety of exercises (e.g. assessing % 1RM for a leg press, lunge, bench press, lat pull down, etc.). Also, strength fluctuates based on a variety of factors, such as how well-rested the client is. Lastly, clients will get stronger over time (with rapid gains in the first few weeks of training), so the original % 1RM will not always match the client’s abilities for a given session. Unless your client is a powerlifter, comprehensive % 1RM testing is unnecessary.
Instead, we can use a target rep range and RPE to achieve that intensity. Aim to work in the range of 6-15 repetitions (2). Loads that can be performed for 6 reps approximate 85% 1RM and loads that can be lifted for 15 reps approximate 60% 1RM. I would recommend starting clients with higher rep sets of 15 and over several weeks working down to lower rep sets of 6, if appropriate and tolerated. However, we won’t be taking sets to absolute failure. Instead, we’ll use RPE to make sure we are working in that 60-85% 1RM range.
2. Use RPE to prescribe and monitor intensity
RPE is a measure of exercise intensity originally developed for cardiovascular exercise, which has since been validated for resistance exercise. There are several valid scales to measure RPE. Here, we’ll use the OMNI Resistance Exercise Scale (OMNI-RES), which has been validated for use in older adults (5). See the figure below with the scale and descriptions of each level.
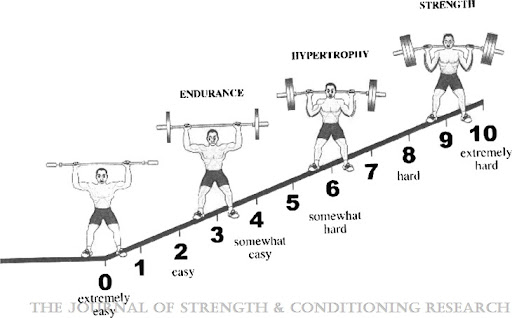
Figure 1. Adapted from Gearhart et al, 2009
First, explain the scale to them and show them a printed version of the OMNI-RES. Then to assess RPE, simply ask the patient to rate their level of exertion at the end of the set. Note that the RPE for light and heavy loads can be the same depending on how close to muscle failure the client gets. Research shows that 30 % 1RM and 80% 1 RM loads had a similar level of RPE when sets were taken to absolute muscle failure (6).
As mentioned earlier, we don’t often want to push until absolute muscle failure. We should work up to an RPE of 6-8 (“somewhat hard” to “hard”) within that 6-15 rep range, to ensure we are applying enough load to get our clients stronger.
Some clients may be started at sets with greater than 15 reps and intensities of less than 6 RPE and that is ok. However, if appropriate and tolerated, they should be progressed into the 6-15 rep range with RPE’s of 6-8 to reach the 60-85% 1RM intensity that is optimal for strengthening.
3. Assess strength adaptations over time

Over time, an appropriate response to strength training is the ability to perform a given rep/load combination more easily. Then because the client has gotten stronger, the reps/load for an exercise can be increased.
For example, a client performs 10 reps on the bench press with 65 lbs at RPE 7. Within a few sessions the client performs the exact same rep/load combination but rates it at RPE 6. The exercise with the same rep/load combination (65 lbs for 10 reps) has gotten easier (i.e. decreased RPE), which means the client has gotten stronger. Since the client has gotten stronger, it would be appropriate to increase the load by 2.5-10%, to accommodate the client’s increased fitness level and keep driving strength gains.
However, if they perform a given rep/load combination for several weeks and the RPE increases (i.e. the exercise is feeling more challenging) or stays the same, this could mean that the client is NOT getting stronger on that exercise. In this case, it might be time to revise the strength training program and/or examine other factors like recovery and nutritional status.
This requires some judgement of how quickly progress should be seen. However, over time the client should be able to perform more reps with heavier loads, with a similar level of RPE.
In addition to measuring the strength adaptations to specific exercises, we should also use functional assessments of strength such as the bicep curl test, heel raise test, and sit to stand.
Wrapping Up
Strength training is vital for the older adult and needs to be properly dosed. To best dose strength exercises you now have three tools:
- Ideal intensity range: 70-85% 1RM, with a rep range of 6-15 reps
- Intensity monitor: RPE, aim for a rating of 6-8 (“somewhat hard” to “hard”)
- Measure of strength adaptations: client response to individual exercises and functional strength assessments
For more on how to design a comprehensive exercise program for older adults take Dr. Wingood’s Masterclass here!
Want to learn how to optimise your exercise prescription for older adults?
Dr Mariana Wingood has done a Masterclass lecture series for us on:
“Exercise prescription for aging adults”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Leave a comment (1)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
yes sir i nice reminder to go to 6-15 reps ; occasionally i have gone over as the start. Nice to know you use RPE too