
I know what your thinking… frozen shoulders and Disney’s animated film ‘Frozen’ is an obvious link, and yes it is. But it’s not just the word frozen that links them, it’s also the infamous song ‘let it go‘ that also connects frozen shoulders and the physiotherapy treatment of them.
I see a lot of frozen shoulders, primary ones with no risk factors, secondary ones with ALL the risk factor, and I also see many who have been told they have frozen shoulder who clearly do not. So first what do I class a frozen shoulder, well that’s simple, thats a stiff and very painful shoulder that has significant and EQUAL loss of both active AND passive movement in most directions, but has a normal x-ray. This loss of movement is classically into external rotation and elevation the most, but it tends to affect all movements, and the pain is severe, diffuse , all consuming and usually unrelenting. All ‘true’ frozen shoulders are extremely painful, extremely limiting, and extremely disabling. When I hear females telling me the pain in their shoulder is worse than child birth, I know I am dealing with a very, very painful condition.
What is a Frozen Shoulder?
Frozen shoulder is a pathology that is still not fully understood. It is an inflammatory condition that affects the capsular tissue of the shoulder, which causes significant neovascularisation, collagen proliferation, fibrosis, and eventual contracture of the capsular, reducing the volume of the shoulder joint significantly. (1)
All frozen shoulders loose significant amounts of movement, as mentioned this is usually in many directions, and can be in differing amounts, but the fibrosis and contractures classically affect the anterior surperior capsule and rotator interval of the shoulder. This limits the big three of reaching over head, reaching out to the side, and reaching behind the back.
Diagnosis of a frozen shoulder, like most things, is usually done mainly with the subjective history. Patients age, medical history, onset, nature, aggs and eases all give clues of a frozen shoulder. Clinical examination to confirm a frozen shoulder is relativity simple, it involves looking for 3-4 movements that have EQUAL loss of both active and passive range of movement with significant pain at end of range, as well as doing resisted shoulder tests that usually produce no significant pain or weakness. This exam usually confirms a frozen shoulder. However many clinicians, myself included, will also ask for an x-ray to check it is normal before they fully confirm a diagnosis of a frozen shoulder.
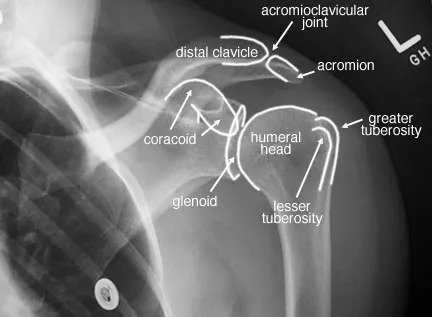
The need for a normal x-ray to confirm a frozen shoulder has been debated and discussed a lot recently, especially on twitter in the last few weeks. The x-ray is first used to help exclude shoulder joint arthritis, however a frozen shoulder and an arthritic shoulder usually have a completely different onset and history. The x-ray has also been suggested to check for sinister pathology that can masquerade as a frozen shoulder (2). However this practice has been questioned recently due to the very low incidence of sinister pathology presenting as shoulder pain, and if a shoulder x-ray is the right tool to check for suspected sinister pathology. I don’t want to dwell on this topic too much, except to say that currently in my practice all frozen shoulders must have a normal x-ray before any treatment can begin.
How do you treat a Frozen Shoulder?
Treatment of a frozen shoulder is extremely varied from place to place, and from person to person (2). There are many options and interventions available with little consensus or evidence on what is best. The options for frozen shoulders range from leave it alone to spontaneously resolve, and I am sure there are many frozen shoulders that do just this. Of course we don’t know exactly how many, or what result they get as we don’t get to see them for follow up.
Other more invasive treatments for frozen shoulder include intra-articular corticosteriod injections, or the increasingly popular, although highly dubious, high volume hydrodilatation injections. Then of course there are surgical options such as manipulation under anesthetic, which unfortunately are still being done despite the high risks of damage such as labral lesions, cuff tears, brachial plexus injury, and even fractures (3). The gold standard surgical procedure for frozen shoulders now is arthroscopic release of contractures.
Physiotherapy is of course also a common treatment for frozen shoulders. This can include massage, joint mobilisations, manipulations, passive stretching, acupuncture, electrotherapy, and exercise (4).
All these treatment options have there pro’s and con’s, and some have more evidence of effectiveness than others. I have my own biases and experiences against many of them. Again I don’t want to dwell on these too much, just to say that a recent Cochrane review for frozen shoulder found that ALL manual therapy and exercise therapy was ineffective in the management of frozen shoulder (5).
And I agree!
In my experience manual therapy and traditional physiotherapy methods for frozen shoulder do very, very little. I have tried them all, pulling and pressing people with painful frozen shoulders, here, there, and everywhere, all with little effect, and all too no avail. I know that some well known shoulder physios disagree with me and advocate deep tissue massage, joint mobilisations, and stretches for frozen shoulders (1), but in my experience these are generally a waste of time, energy, and resources, and more importantly they only tend to cause patients unnecessary pain and distress for very little benefit.
However, there is a ‘different’ method for treating frozen shoulders that I have been using more and more over the years, which not only do I find far more effective, and far more tolerable for patients than ‘traditional’ physiotherapy, but more importantly it can be done independently, simply and easily by the patient with out a physio inflicting torture on them.
This is where my connection with the song ‘let it go’ comes in.
So what is this method of treating frozen shoulders? Well its using eccentric loading. Eccentric exercise has been shown to have many benefits in the management of many musculo-skeletal conditions, however they are not routinely used in the management of frozen shoulders, I think they should be.
One of the known benefits of eccentric exercise is improvements in joint flexibility via the processes of sarcomerogenesis. This is the physical addition of individual sarcomeres to musculotendinous junctions. This has been shown to produce a physical increase in the length of connective tissue, and so improves range of movement. Sarcomerogenesis has been shown to occur in the lower limb very quickly, very simply, and very easily. In fact eccentric loading has been shown to produce significant improvements in range of movement in far less time, and with far less energy than traditional stretching, and of course you also get stronger (6)!
Effect of eccentric v’s concentric exercises on increase in hamstring muscle length within two weeks (7)
Warning: Anecdote alert ahead!
I have been using eccentric exercises with all my frozen shoulders after reading the effect they have on the lower limb a few years ago, and I have found patients find them not only more effective but simpler, easier and less painful to do than traditional stretching, and more importantly they seem to be more effective than ANY other kind of manual therapy I have used in the past.
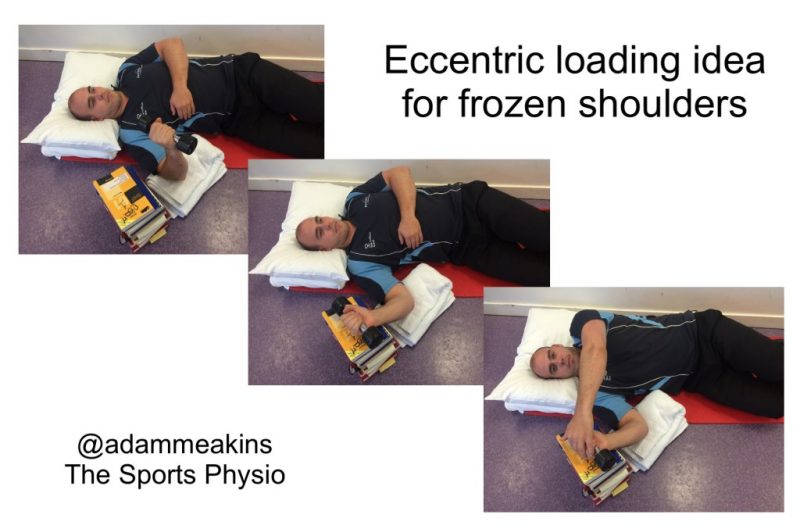
There are a number of ways eccentric exercises can be done for frozen shoulders. The way I usually like to do them is to get the patient lying on their back. Then to hold a weight in their hand as they lower the weight slowly into external rotation towards a target that has been set just within their available tolerable range (a stack of books work well here).
They then return the arm to the start position, maybe using their other hand to assist on the concentric phase if needs be. They do a few reps and when the shoulder starts to feel ‘looser’ the target is adjusted and lowered by removing a few books to allow a little more movement to occur, a few more reps are completed, then the target re-adjusted again and so they continue as tolerated.
I usually ask patients to do the reps slowly, the slower the better, and with a weight that is challenging to control down, but not too heavy as to feel ‘out of control’ or too painful. I usually dont give a fixed number of sets or reps, rather I ask them to do as many as they can. I like to ask most to try ans do 3 sets in a row with a few minutes rest inbetween, but this is adjustable depending on the individuals pain and tolerance.
Now I am not sure if the physiological effects of eccentric loading on the shoulder like this will be the same as seen in the lower limb as the loads used will be a lot lower, and so I am not convinced if the physiological stimulus will be enough to produce similar physiological adaption to occur such as sarcomerogenesis.
There is also very little research on eccentric loading and sarcomerogenesis in the upper limb. One paper did show some changes in the myofibril length when eccentric training was compared against concentric, but it was a small study on healthy individuals and not that conclusive (8), but it’s all I could find.
However, anecdotally when I use eccentric exercises like these on frozen shoulders I only see some really good results and marked improvements in range of movement and pain, very quickly, and I mean very, very quickly, usually within one or two sets, some times even within a few repetitions.
Now I am not for one minute suggesting that these immediate changes in range of shoulder movement are due to any mechanical or biological changes in the tissue, that just doesn’t happen that quickly. However, what I do think is happening is a couple of things.
First is the well known hypo-analgesic effect of exercise allowing the patient to become more tolerant to the exercise (9). I also think other psychological effects are at play when doing a resistance exercise with a painful body part. To begin with it can be a bit daunting and scary, but when done a few times and the patient realises and is reassured that they don’t cause more pain, and in fact they reduce it, this allows the protective, reflexive muscle guarding and increased tension of the shoulder muscles to… ‘let go’
Pain is a protective response. Pain causes muscles to guard. Frozen shoulders have a lot of pain. Frozen shoulders have a lot of muscles guarding. Eccentric exercises in my opinion helps these guarding muscles to ‘let go’.
I often like to use analogy’s to help patients understand the mechanisms of therapy effects where possible. One that works well for eccentric exercises is one I have ‘borrowed’ from Prof Peter O’Sullivan that he uses on his CFT workshops. This is by using a clenched fist as a metaphor for the shoulder muscles being tight and guarded. I demonstrate and explain with a clenched fist that this is what the pain causes the muscles around the shoulder joint to do, and these exercises start to ‘let it go‘ so the movement can improve. See Pete’s similar demo on a chap with low back pain here (10).
As far as I am aware there is no direct evidence for the use of eccentric loading exercises for frozen shoulders, but I do think this is something that needs to be looked into, and so I have started case study recording data of a group of frozen shoulders over 3 months.
Now, you may also be thinking why am I using a strengthening exercise for a frozen shoulder, which is not a contractile dysfunction but rather a capsular issue.
Well that’s because the capsule of the shoulder and the rotator cuff are one and the same structure. Anyone who has seen shoulder anatomy with there own eyes will tell you the rotator cuff and the capsule are blended structures with no clear differentiation, and although they have different roles in the shoulder, they are essentially the same structure.
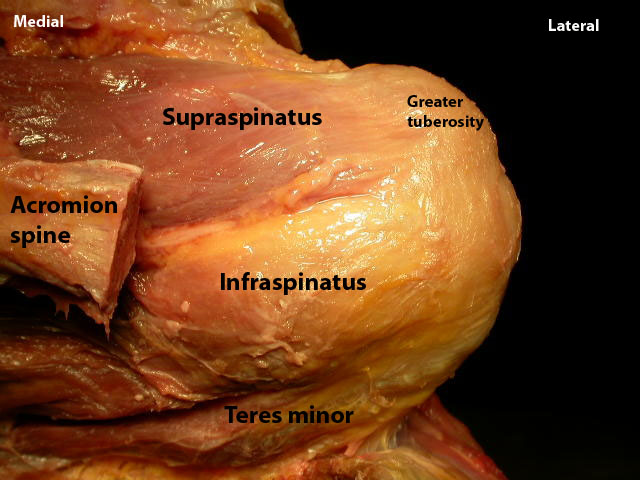
It must be remembered that the rotator cuff acts directly on a shoulder capsule by pulling on it to move, rotate, and stabilise the humeral head. So any contraction of the rotator cuff will place tension on the shoulder capsule, and so repeated tension and exercising of the cuff will have a repeated tension affects on the capsule tissue as well.
So The next time you have a patient with a frozen shoulder try using some eccentric loading exercises, and see for yourself how simple, easy and effective they can be. Of course you can supplement these with other modalities if you want. I don’t. I like my patients to do these, and then do some more of these, and then do some more of these, for the whole session, in various positions and angles.
Also try explaining to your patient’s with frozen shoulders to ‘let it go, let it go…‘ and try using the clenched fist analogy. However, breaking into song as you do this is entirely optional, but occasionally I do find that it helps with some of my patients, they are either to stunned or shocked at my singing to realise that they have just let their shoulder… ‘go‘
I don’t mind the cold anyway…
As always thanks for reading
Adam
Learn more from Adam HERE.
Want to become more confident treating the shoulder?
Dr Angela Cadogan has done a Masterclass lecture series for us!
“Frozen Shoulder–Unravelling the Enigma”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Leave a comment (2)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Sehr Interessant!
Dankeschön
Wow, this has to be the best article I’ve seen on ‘Frozen Shoulder’ thus far.
I loved everything about the article. I’m an undergraduate student of Physiotherapy, and I really do appreciate the efforts you put into this article. It was so easy to read and very understandable. I loved how you made it so relatable as well. Thank you Adams!