Have the butt muscles of the world gone silent?

From my extremely unscientific observation it appears that 67-74% of my patients have been told their glutes are inhibited and don’t work properly. It seems to be an epidemic. I had to cancel my Runner’s World subscription because the onslaught of glute inhibition articles was too depressing and I chose avoidance as my coping mechanism.
Open a fitness magazine and you will read quotes like this:
Because we sit on our butt all day, it sometimes forgets what it’s supposed to do when we go to run. Source here
You hear that? Your Glute muscle “forgets” what to do? This concept is pretty rampant in the fitness and health world. You’d think there was a lot of research to support it. TL:DR – there isn’t.
There is the idea that the Gluteus Maximus is a muscle prone to becoming inhibited. Meaning, it tests weak but it has the potential to be strong if only the person could learn to “turn it on”. It is also commonly suggested that that inhibition will also lead to a weak muscle in the future
These ideas started with Vladimir Janda decades ago and are assumed to manifest themselves in a postural position called the lower crossed syndrome. This sees the person with “tight” hip flexors, tight erector spine, “long” and weak abdominal muscles and weak Gluteus Maximus muscles. So, essential people have argued for the existence of something (Glut Max not turning on) with a dysfunctional postural theory (the lower crossed syndrome) that does not exist either. Its like hearing about a Unicorn parade from my 5 year old when her source was the Tooth Fairy.
The idea that many people have inhibited Glute muscles has essentially become a truism and yet it doesn’t have a lot of research support for it. I would argue two things:
1. the Glutes are no more likely to become inhibited than any other muscle that we possess and
2. that the Glutes are no more important than other hip extensor muscle.
We really don’t need to elevate the importance of one muscle over another and I don’t think we need to create pathology where one doesn’t exist. Many of our patients feel broken enough without adding on imaginary dysfunctions.
I might sound jaded – I’m not, I’m just tired. I have been banging my head against this supposed dysfunction since 2004! 15 years! We wrote a paper (here and blog here)looking at the concept of the Gluteus Maximus being inhibited and found that it is “inhibited” or late to turn on in everyone. Meaning, what people were calling a dysfunction was just normal existence.
Diagnosis: HUMAN
Anyways, the point of this blog is to explore the ideas behind the concept of inhibited Glutes. Look at some of the research and even try to find out when the idea might be relevant to people in pain.
Is less Gluteus Maximus activity related to pain and injury.
There are plenty of research papers where we see MORE Gluteus Maximus activity in the presence of pain and injury. Here are a few:
– Decreased Glute Max activity when you do a symptom modification procedure to the SI Joint and INCREASED Glute Max activity in the painful group. Paper here
– My old and uninspired research (2004) showing Glute Max is always delayed during the prone leg lift. Repeated by many since then
– Prospective, accidentally, case study research showing that a sub-elite athlete’s ankle sprain doesn’t lead to delays in firing (my wife was the patient – we had her “normal” EMG and she luckily sprained her ankle for me 🙂 – that is true love
– Onset times of those with Low Back Pain are not delayed in the Glute Max. Paper here
– Increased Glut Medius activity associated with increased pain during standing. Paper here
– Those with hip OA showing INCREASED Glute Medius activity. Paper here
– Hold on this one is crazy. Experimentally induced Glut Med weakness does not lead to increased knee Adduction moment (the thing sometimes linked to joint degeneration progression but not always pain). Paper here
– No difference in glute max activity in those with low back pain…again. Paper here
– Increased Glute Max activity in those with hamstring strains. Paper here
– In a prospective study it was a delay in the HAMSTRINGS that was associated with an increased risk of hamstring injury. Paper here
Some dissenting studies – suggesting gluteal inhibition exists.
– a very interesting study where we see here that injecting fluid into a sensitive hip joint capsule will lead to less Glute activity during a hip bridge exercise https://www.ncbi.nlm.nih.gov/pubmed/23261019
One thing about the above study was that there seems to be more activity in the painful hip compared to the non-painful before the fluid is injected into the hip. So, while it appears that arthrogenic inhibition may have occurred it essentially “normalized” the activity (although, we should all be careful with comparing EMG amplitudes between different people and even between different sides of the body – great paper here that I was lucky to be a part of). As the muscle activity just seemed to approximate that of the normal hip. So, does this study actually tell us if gluteal inhibition exists? You can almost use it to argue again that there is more muscle activity in the painful hip.
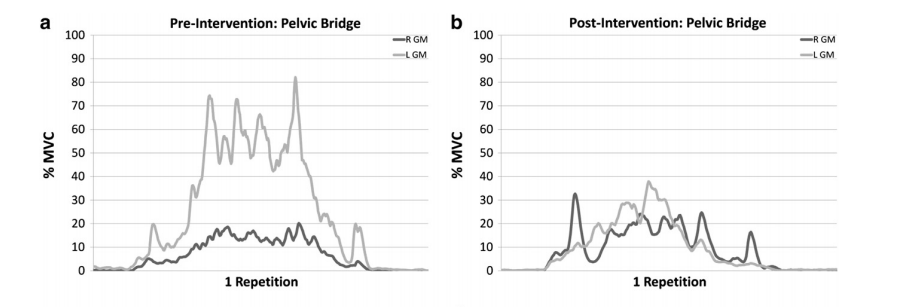
After hip joint injection we see a decrease in Glute Max activity during a hip bridge (Freeman et al 2013)
Another prospective paper. These authors suggest that sprinters who sprint with greater Gluteus Maximus activity during the later half of the swing phase are less likely to experience a hamstring strain
https://www.ncbi.nlm.nih.gov/pubmed/28263670
Are the ideas behind Gluteal Inhibition plausible?
One tenet of gluteal inhibition is that supposedly tight hip flexors cause the glutes to not fire as well because of something called reciprocal inhibition. Which is essentially a reflexive phenomenon where if a muscle is “turned on” to fire, our nervous system will try to inhibit the opposite muscle from firing at the same time. This is probably most pronounced during walking because while we want some muscle contraction to stabilize a joint we don’t want muscles “fighting” against one another as we walk because this would be inefficient.
Where this idea falls apart when it comes to the Glutes is that it assumes that because a muscle or joint has decreased range of motion (e.g the hip flexors are “tight”) that these muscles have some sort of extra muscle activity that causes that tightness and this in turn inhibits the antagonist (i.e. The Glutes). This is a really unsupported idea and doesn’t make sense. “Tight” muscles don’t usually have extra muscle activity (or a lot more, if any) – especially at rest or when they shorten. You can see this when someone squats. Squats are relevant because many say that a “tight” psoas will inhibit the Glute Max and this a problem during squatting. However, when you squat, your hip flexors become slackened. The hip flexors are NOT working to flex the hips. Gravity is doing that. The Glutes are essentially “lowering” you to the ground because gravity is “flexing” your hips not your hip flexors. A “tight” hip flexor would not influence your squatting mechanics and would not be “turned on” anymore than if you had very mobile hips.
Another critique against the concept of gluteal inhibition being relevant to pain is that we have made the Glutes more important than they actually are. Ask yourself this “Even if the glutes are inhibited why would that be a problem?” You don’t really need a lot of Gluteus Maximus activity to do the vast majority of daily tasks. Your glutes work during heavy load end range activities. Think sprinting, climbing or lifting heavy. You just don’t need a lot of glute activity to walk or even run. Have a look a the Dorn paper on running in 2012. It’s the calf muscles that really drive running. The hip extensors just aren’t that involved. This is also supported by the work of Rich Willy more recently where they showed that the majority of the total support moment comes from the ankle and knee with the hip playing a small role.
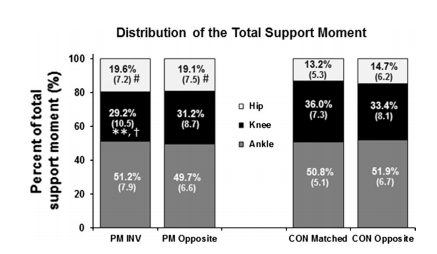
Willy et al 2017
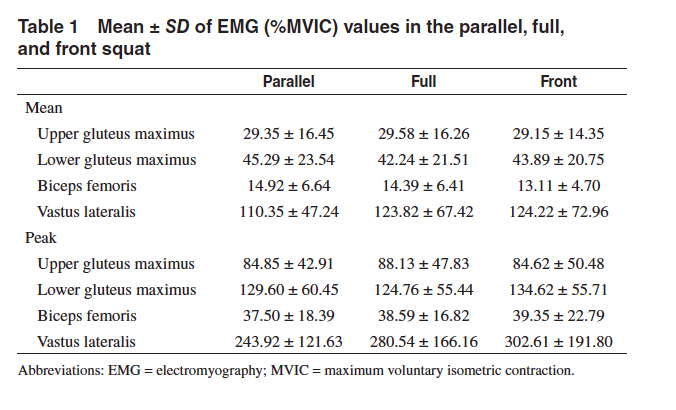
You can also see this in Bret Contreras’s studies on Glute activity during squatting. Even in these high load activities we don’t see maximal glute activation.
Disclaimer of Bias and Difficulty with this Discussion
1. Glute muscles can certainly become weak.
As can many muscles when we have pain or sedentary behaviour. Weakness is a factor in some injuries and is certainly something important to address for performance.
2. Can we salvage the concept of gluteal inhibition?
I think so. It just requires us to move away from describing how people move as dysfunctional and avoiding unnecessary complications. I think it is possible to move in a way that does not require a lot of Gluteal activity. Meaning you could certainly lift something from the floor that is more of a spinal or knee dominant pattern. You can certainly tweak your technique to use your hips more if you so chose. The other patterns aren’t inherently wrong they are just different movement patterns. And if those patterns are sensitive it is certainly reasonable to learn to move with a more hip dominant pattern. See, that is simple. We don’t need to follow any dysfunction junction reasoning here.
Another more complex and extremely debatable example might be seen with a high load activity like sprinting (not an expertise of mine). At high loads your hamstrings will undergo high strains. The Glutes are certainly hip extensors during sprinting and I would assume (because this hasn’t been tested) there are running technique changes that might allow you to bias the hip extension torque production to a greater role of the Glutes. Potentially, this might decrease the strain on the hamstrings. This might be relevant for hamstring injuries. Have I used the word “might” enough?
When the above scenario would not be relevant is any painful condition where high forces and true tissue injuries are not the driver of dysfunction and pain. This would be something like jogging or walking. You just don’t need a lot of Glute activity when you jog and its unlikely that a lack of gluteal activation is what is causing the pain problem. Weakness of the hips might be relevant but there is no reason to think people in pain are somehow not “accessing” their hip extension producing capabilities when they jog.
3. Is addressing Gluteal Strength Helpful?
I want to reiterate that the practice style that “dead butt syndrome” spawned can certainly help a lot of people. In general, it leads to increasing physical activity, resistance training for the hips, spine or legs and often involves changing postures/movements to symptom modify. There is often nothing wrong with any of that. Strength training the hips certainly has pragmatic evidence to help people with knee pain. It should be something we do.
But, clinical success does not prove a mechanism. Instead of us thinking that people have inhibited glutes we can look at the treatment approach in another way. If someone has low back pain that is associated with flexion its reasonable to teach them to lift or move temporarily with less lumbar flexion. This will require moving more through the hips (a hip hinge) and we can reinforce this new movement pattern with hip exercises that involve the glutes and move the spine less. GREAT. Fantastic, we’ve taught someone to avoid a sensitive position and then loaded them up which can be an analgesic, given them some control of their pain and started them on an activity program. All things helpful for pain. Teaching people to move differently and try to bias their hip extensors can be a great way to decrease the load on the knee, to decrease the load on the spine and to help people move differently and without pain. What you do clinically can still be helpful but it doesn’t prove the idea of there being a pathology with the Glutes.
But, again, it does not mean they had some dysfunctional gluteal firing patterns. We just avoided a painful position temporarily and prescribed exercise. Easy-peasy.
This is concept is not new. We’ve seen this shift from “fixing” assumed dysfunctions to simply doing symptom modification and maximizing function at pretty much every other joint (Shoulder would be here).
Wrap it up
To end, please strength train the hips if you think its helpful, for health, for life, for performance. The entire hip. It certainly has pragmatic evidence to be helpful for some. But, perhaps we avoid telling people how dysfunctional they are. Again, lets build people up instead of knocking them down. And if in doubt…
This was originally posted on Greg Lehman’s website. You can click here to read more blogs from them.
👩⚕️ Want an easier way to develop your assessment & treatment skills?
🙌 Our Practical video sessions are the perfect solution!
🎥 They allow you to see exactly how top experts assess and treat specific conditions.
💪 So you can become a better clinician, faster.

Don’t forget to share this blog!
Leave a comment (1)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Interesting article! I am guilty of telling people they have weak/inhibited glutes and tight hip flexors. We definitely need to stop spreading thought viruses and focus on empowering our patients and getting them stronger and more fit