Clinical Pearls for Diagnosing Hip and Groin Pain in Adolescents

Hip and groin pain in sporty adolescents is not normal.
We can be a bit more relaxed in adults and allow them some aches and pains. We invariably develop degenerative changes into our middle and late ages. But – kids aren’t ‘little adults’ – they have different physiology. Crucially, they are susceptible to unique conditions.
Yet, they are robust (how often do you see child athletes in clinics?). If they are in pain and not enjoying sport, it’s very important to pay attention and explore why. This blog will outline some key features to look out for in adolescents.
Apophyses
Apophyses are the ‘anchors’ for the muscle-tendon unit. Adolescent athletes are increasingly highly conditioned particularly in contact sports such as rugby. They essentially possess adult musculature, developing impressive forces across an immature skeleton. This leaves the apophyses prone to injury. The physeal cartilage is weaker than tendon and muscle. Therefore, the ‘anchor’ can fail before the ‘rope’ (Figure 1).
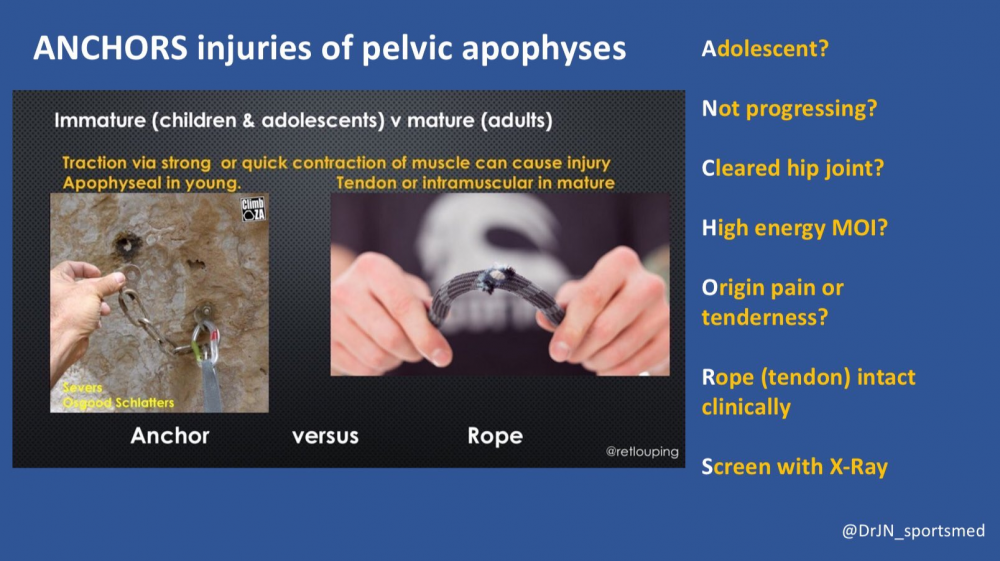
Figure 1 – ANCHOR Injuries
Child athletes rarely tear muscles or develop tendinosis, so be wary of applying these diagnostic labels and ask yourself if you are overlooking an apophyses injury.
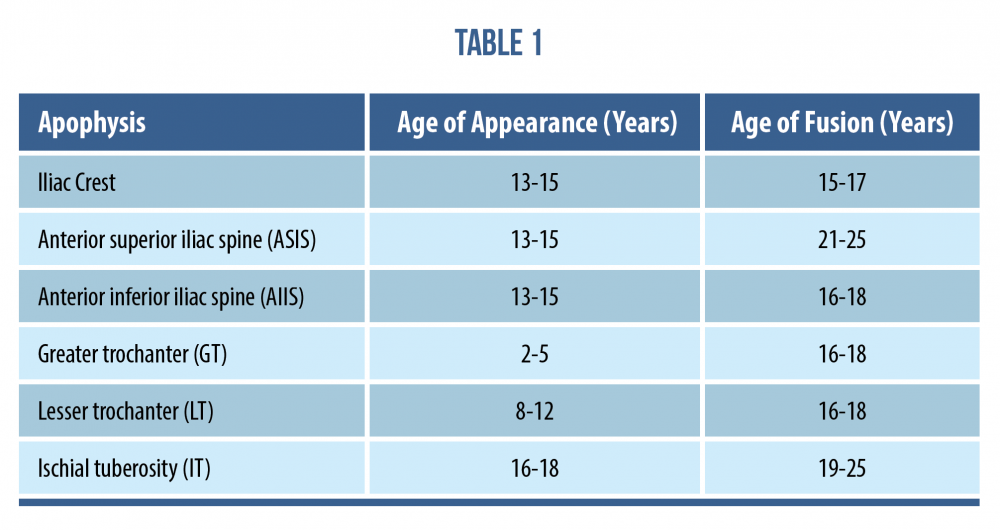
The pelvic apophyses appear, then fuse, at variable ages. Notably the ischial (hamstring origin) and anterior superior iliac spine (Tensor Fascia Lata and Sartorius) sometimes ossify well into late teens and early 20s. Pubic apophyses can be as delayed as late 20’s! See Table 1 below and bear this in mind even if you think you are treating an adult.
Case Study 1
Here is an example of this in a late teenage footballer. Central pubic and lower abdominal pain radiating into bilateral medial groin adductor region. The axial oblique MRI images (figure 3 and 4) show pubic apophysitis with oedema and mild fragmentation of apophyses. It is an unusual diagnosis but worth bearing in mind in younger patients playing multi-directional demand sports with adductor or pubic related groin pain.

Figure 3

Figure 4
Apophysitis
Apophysitis (overload of the immature growth plate leading to micro-stress and inflammation) can affect numerous pelvic sites (figure 5 [1]).
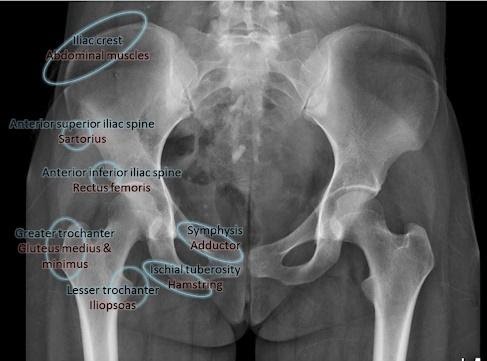
Figure 5
Many consider it equivalent to tendinopathy, but often it fails to ‘warm up’ and the adolescent struggles to maintain performance, including describing power loss or heaviness. Maybe it has more in common with a bone stress injury? Patients can also get discomfort at rest and at night when severe.
It’s invariably training error driven, so explore this in detail – take the time to quiz the parents about introduction of new sessions, drills and playing up at higher age groups. Is there a new coach with a different training ethos?
Apophysitis can cause variable and diffuse radiating pain patterns which can be confusing. They may mimic lumbar spine referral, for example rectus femoris (anterior inferior iliac spine; AIIS) beyond the groin, into thigh and hamstring origin (ischial tuberosity) into buttock, perineum, and posterior thigh.
In an over-training child athlete, they can co-exist, ‘muddying the clinical waters’ further! Below is a relevant case study with this in mind.
Case Study 2
Mid teen footballer presenting with bilateral inferior gluteal, proximal hamstring and medial groin pain. This was accompanied with an increased training intensity with new step over and pivoting drills. MRI showed bilateral ischial apophysitis (bone marrow oedema arrowed in figure 6 and 7) and adductor origin inflammation (not shown).

Figure 6
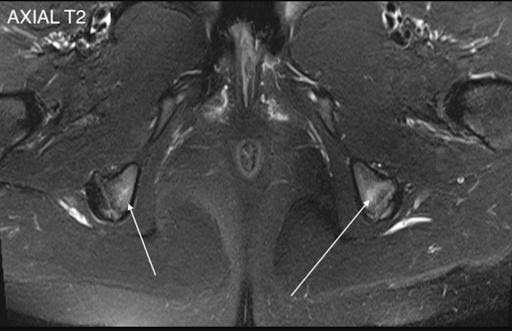
Figure 7
In these multi-site cases we should also have rheumatological causes at the back of our mind. ‘Inflammatory’ conditions affect children as well as adults!
Apophyseal Avulsion
Growth plates can also be acutely injured – a traumatic avulsion fracture – typically caused by a rapid, explosive contraction of the parent muscle with the energy transferred to and overcoming the apophysis ‘anchor’.
Often the patient has complained of pain for some time preceding the event which is due to apophysitis (i.e. it’s already vulnerable and the threshold for acute injury is lower).
It won’t be a muscle tear especially if close to the pelvis. Don’t miss these. Have a low threshold for imaging; X-ray is a fantastic start, will cover most evils and are easily accessible for most.
Case Study 3
The below X-ray (2) and ultrasound images are from a young teen footballer with an acute, painful ‘pop’ over the high left lateral hip on landing from a jump.
He struggled to bear weight and retired. Examination revealed him unable to single leg squat, Tensor Fascia Lata loading and oblique crunches were sore; exquisitely tender with swelling over 8cm of the iliac crest to the anterior superior iliac spine.
Figure 8 and 9 revealed avulsion of the iliac crest apophysis – rare!!

Figure 8 – AP pelvis xray
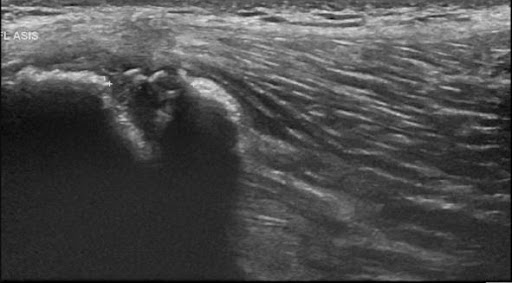
Figure 9 – Ultrasound iliac crest
Below are 2 examples of how missed avulsion injuries can cause issues longer term.
Case Study 4
The mechanism of injury involved a forceful football kick, placing rectus femoris under high load, leading to avulsion of AIIS (figures 10 and 11).

Figure 10 – AP pelvic x-ray
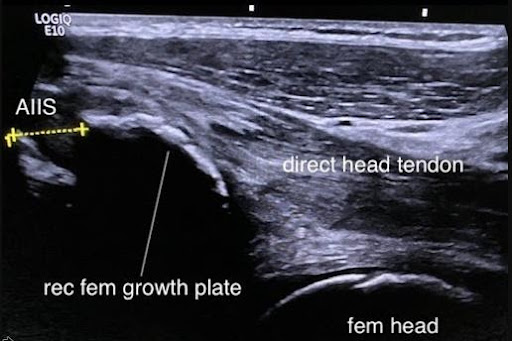
Figure 11- Ultrasound AIIS
Progressive heterotopic calcification of the displaced apophysis and scar (subsequently demonstrated on CT scan), led to subspinous hip impingement and marked loss of sporting function and range of movement.
Case Study 5
The mechanism of injury involved a sudden explosive sprint effort causing a massive avulsion of ischial tuberosity, including a part of the bony origin (see figures 12 and 13).

Figure 12

Figure 13 – MRI coronal right hip
This was treated as a hamstring tear for approximately a year. The young teenager subsequently developed disabling sitting pain interfering with studies as well as sciatic nerve irritation due to local compression. If this was identified early it could have been treated surgically.
Apophyseal Treatment
Follow basic rehabilitation fundamentals by calming things down, offloading, gradually build load, seek to improve capacity, consider sports specific needs and address strength deficits and potential technical errors. Particularly for avulsion injuries, it is wise to avoid early stretching. It’s crucial to set realistic timescales, as is consistent communication with parents, the school and coach.
Invariably, these talented young athletes will be playing multiple sports; you may need to suggest the patient stick to their favourite sport in the short to medium term. It may also need to become a permanent change. Listen to what the young athlete wants; it’s not necessarily the same as the parents! Ultimately if the training error isn’t addressed, there’s a strong chance they will become frustrated by recurrent or persistent injury.
The adolescent capacity for healing is insane – respect the physiology and embrace it. Don’t attempt to leapfrog it.
Is it Something Else?
It’s not always the apophyses.
Be vigilant for childhood conditions such as Perthes diseases in 5-10 year olds (see figure 14 [3]) and Slipped Upper Femoral Epiphyses in 10-15 year olds (see figure 15).

Figure 14

Figure 15
Missing these can condemn the child to accelerated loss of function, osteoarthritis, and early hip replacement in adulthood. They need orthopaedic input. Again, have a low threshold for imaging.
Do they present with medial knee pain? Be suspicious of the hip causing referred pain. It takes a few seconds to screen the hip in a consultation.
A medicolegal ‘no-brainer’.
Tumours
Be wary of primary bone and soft tissue tumours in the proximal femoral metaphysis and the pelvis. It is a bit of a ‘hot spot’. Do they have night pain? Is it unrelated to activity? Progressive? If so, x-ray please!

Figure 16
Labral Tears
Although these are less common in kids, they’re much more likely to be symptomatic. We know how common they are incidentally in the adult population.
If you suspect one you need to ask why it’s happened. It’s typically secondary to morphological changes such as Femoroacetabular Impingement or Hip Dysplasia. See the case study below.
Case Study 6
Here is a 13-year-old male footballer with professional aspirations. They developed acute onset left groin pain while sprinting (on the back of a sustained period of increased training intensity), failing to settle several weeks down the line. They had preceding grumbling, but manageable, buttock pain and intermittent clunking.
MRI demonstrated an anterior labral tear, but also lateral acetabular ‘under coverage’. The subsequent CT with 3D reconstruction images (Figs 17 & 18) – the gold standard investigation – shows dysplasia principally of the posterior wall.

Figure 17 CT (anterior view)

Figure 18 – CT (posterior view)
Kids with Dysplasia Need to be Recognised
These patients may be labelled as ‘hypermobile’, with pain at the outer range of motion passively. They may complain of groin, lateral hip, or buttock pain. The ‘hip cuff’ muscles are working overtime to compensate for the low-level instability. Don’t be fooled into labelling it as a ‘hip flexor’ or ‘glute’ problem and hammering away treating it as such. If you think it’s a muscular driver, think harder about what might be underpinning it.
Children with moderate to severe dysplasia (4) may benefit from surgery such as a pelvic osteotomy to preserve the joint. Get an x-ray (figure 19)!

Figure 19
Parents
“Coach says they could go all the way”.
Be vigilant for parental pressures. The vast majority of parents have their child’s best interests at heart. However, lack of education around injury management, misplaced enthusiasm and vicarious drive can facilitate overuse injury. Encouraging multiple sports in and out of school, extra skill / S&C sessions to give the child the competitive advantage can create the injury ‘perfect storm’.
Ask the patient if they’re enjoying their sport. If possible, get them on their own to chat (maybe in the rehab gym). Otherwise, they will tend to say what they think their parents want to hear!
If an adolescent injury is vague, the story or examination inconsistent, imaging unremarkable, they are withdrawn or quiet in the consultation, be mindful that in rare cases their ‘injury’ could be their outward physical expression of psychological distress.
Summary
This blog can be summarised with the following 5 points:
- Kids don’t get muscle or tendon injuries – think apophyses.
- Image early – x-ray!
- Be vigilant for red flags and childhood conditions.
- Engage parents and observe their influence.
- Kids love their sport – it’s socially defining – if they are unhappy, there’s a significant problem.
Want to learn more about the groin?
Dr Andrea Mosler has done a Masterclass lecture series for us on:
“Groin pain in Athletes: unraveling the mystery”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!