How to assess and treat two major causes of dizziness

Dizziness is one of the major complaints in our elderly population. It is often multifactorial and complex to treat. Benign Paroxysmal Positional Vertigo (BPPV) and Peripheral Vestibular Dysfunction are two big causes of dizziness and people with these diagnoses are frequently referred for physical therapy. Though these conditions both cause dizziness complaints, the pathophysiology and treatment are very different. In this blog, you’ll learn to distinguish them as well as treat them properly.
If you’re interested in this topic, I highly recommend you watch Vanessa Simpson’s Masterclass on Vestibular Dysfunction: From Assessment to Rehabilitation.
BPPV
BPPV is the most common cause of dizziness. Typical symptoms include a spinning sensation that is typically brief (<1min) and triggered by changes in head position relative to gravity. People who experience BPPV do not get hearing loss or tinnitus but can encounter additional symptoms like nausea, vomiting, blurred vision, headache, neck pain.
There are two questions that have high diagnostic value when it comes to BPPV:
- Does the patient experience dizziness when lying down/turning in bed?
- And how long does the vertigo episode last?
If your patient has BPPV, the answer to the first question will almost always be yes and the spinning episodes will usually be rather short, from a couple of seconds to a maximum of one minute.
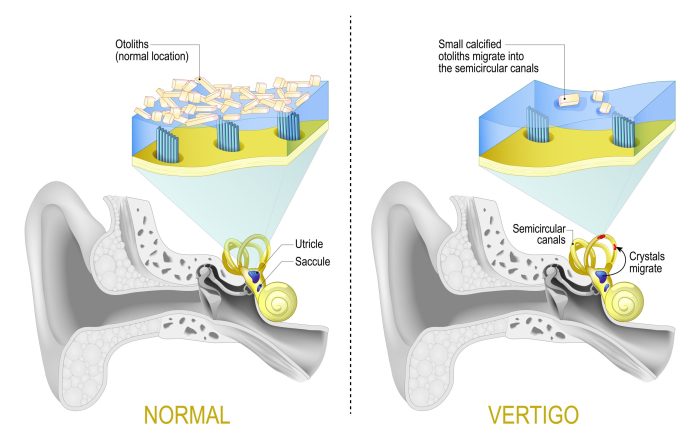
Mechanism
So what exactly causes this spinning sensation? Small calcium carbonate particles called otoconia break free and fall into one or more of the semicircular canals that are part of our vestibular system. This results in an abnormal overexcitement of the hair cells when the head is moved. The vestibular nerve picks up this stronger signal and sends it to the brain, which then gets confused because it is getting other information from the left than from the right side. The result: vertigo.
Assessment
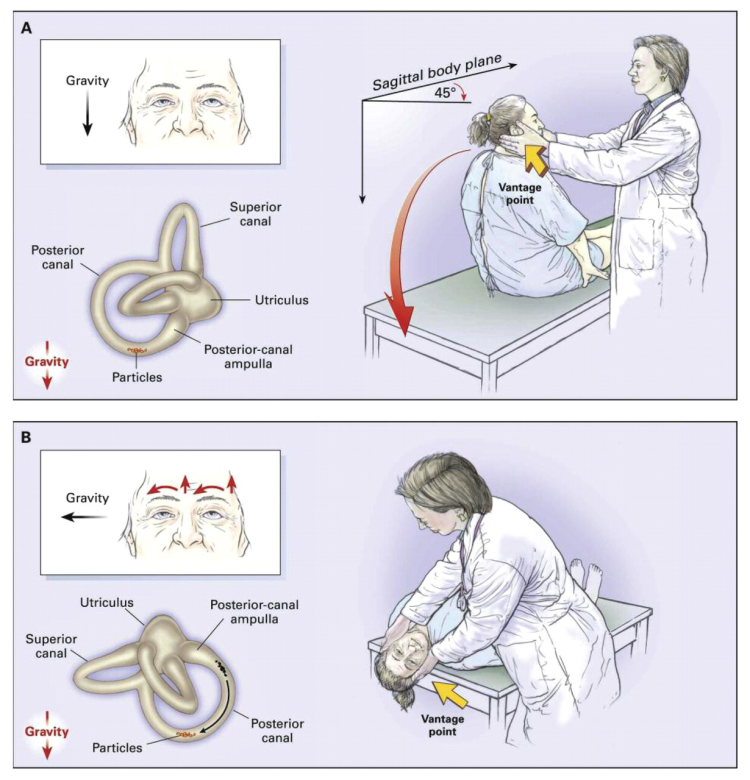
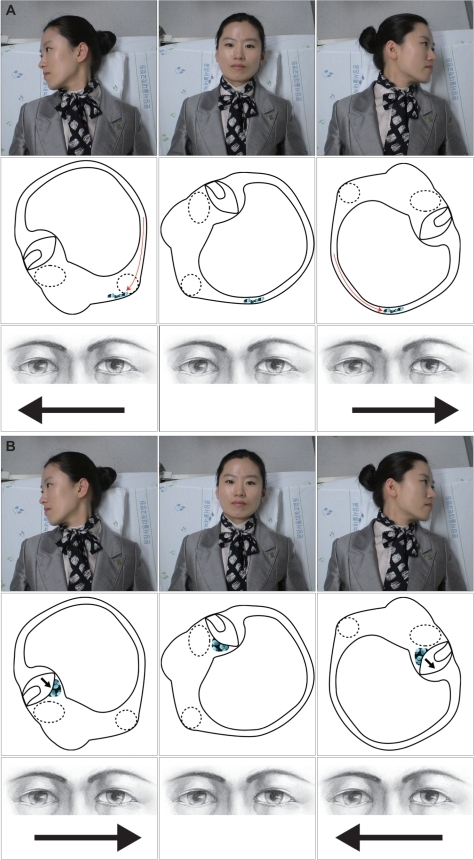
There are multiple tests you can use to diagnose BPPV. Different tests will target different semicircular canals. The well-known Dix Hallpike test and lesser known side lying test will pick up BPPV caused by particles stuck in the posterior and anterior canals. The horizontal canals require a different kind of testing, as their orientation differs from the anterior/posterior canals. The Roll test is the most accurate test to screen for BPPV coming from the horizontal canals. A test is positive when a rapid, involuntary eye movement called nystagmus appears. The direction of the nystagmus will depend on which canals are affected.
Treatment
Dizziness caused by BPPV goes away when the calcium carbonate particles are removed from the semicircular canals. Fortunately, this doesn’t require surgery as there are a number of different maneuvers you can use to move the particles out of the canals.
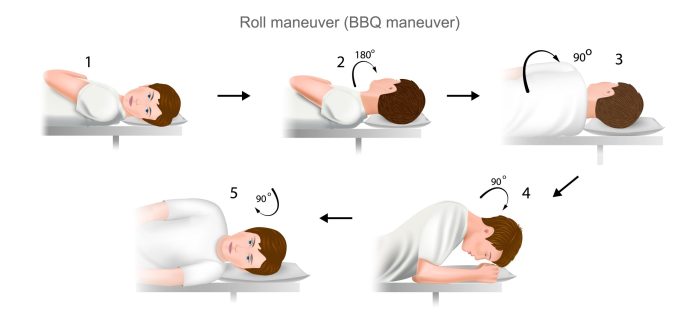
Like during assessment, which maneuver you use depends on the canal that is affected. The modified Epley Maneuver will best remove particles from the posterior canal, while the BBQ Roll is most effective for horizontal canalithiasis.

Peripheral Vestibular Dysfunction
Peripheral Vestibular Dysfunction (PVD) is caused by damage to the vestibular system which is located in the inner ear. Sensory cells in the vestibular organs fail to send signals to the brain correctly, which then gets confused and causes vertigo, visual disturbance and loss of balance. Damage can either be complete or partial, uni- or bilateral and will determine the experienced symptoms.
Unilateral Vestibular Loss (UVL) comes with vertigo, nystagmus (mostly horizontal and towards the unaffected ear), nausea and imbalance and can persist for 3-4 days even at rest with the eyes closed. These patients often visit the emergency department and may require bed rest, medication and fluids. After a couple of days, the brain begins to compensate for the altered neural activity. Symptoms therefore change slightly. There will be dizziness and visual blurring on rapid head movement, imbalance, a feeling of lightheadedness and disorientation that can last for hours, but no more nystagmus.
In cases of Bilateral Vestibular Loss (BVL), the brain doesn’t receive any signals from both balance organs, which means there isn’t any contradictory information and therefore no dizziness, vertigo or nystagmus. Patients do experience severe oscillopsia, which is the apparent movement of a still environment induced by head movement, as well as severe imbalance or walking impairments and general lightheadedness.
Assessment
There is no one specific diagnostic test for PVD. Ocular motor testing to differentiate whether the problem is central or peripheral, positional testing to check for BPPV and the dynamic visual acuity test to check the vestibulo-ocular reflex are general vestibular tests that should always be part of the objective examination of a person who complains of dizziness.
The head impulse test and head shaking nystagmus test are two very valuable tests that can identify peripheral vestibular deficits. Both tests screen for involuntary eye movements.
The Clinical Test of Sensory Interaction on Balance (CTSIB) is another valuable test to screen for Peripheral Vestibular disorder. It was developed to assess sensory contributions to postural control. The vestibular system, our vision and somatosensory system must correctly work together in order for us to obtain our balance. The CTSIB will test all of these 3 systems together, altering each input (except the vestibular input) by removing vision or adapting the standing surface.
Treatment
Treating vestibular loss caused by peripheral vestibular dysfunction is a lot more challenging than treating BPPV. Patients MUST move and challenge the brain and inner ear system, which means they must get dizzy to improve. It is very important to educate your patients about this, as they’ll instinctively try to avoid anything that provokes their dizziness. Adaptation, substitution and gaze stability exercises play an important role in the treatment of vestibular loss and should be performed multiple times per day.
Wrapping up
Hopefully, the world of dizziness has become a little less daunting after reading this blog. If you want to learn more about this topic, make sure to watch Vanessa Simpson’s Masterclass here.
Want to become more confident treating vestibular disorders?
Vanessa Simpson has done a Masterclass lecture series for us!
“Vestibular Dysfunction: From Assessment to Rehabilitation”
You can try Masterclass for FREE now with our 7-day trial!

Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!