Iliotibial Band Pain in the Runner Part 2: Treatment

This is the second of a two-part series by Rich Willy, PT, PhD, on Iliotibial band (ITB) pain. ITB pain is common in runners but there is little guidance in the literature for treating this tricky injury. In Part 1, the etiology of ITB pain was discussed. In Part 2, we discuss treatment for this injury.
Small print: This blog provides an update on the literature around the treatment of runners with ITB pain. It is not medical advice. If you have knee pain with running go see a qualified clinician for proper examination and treatment!
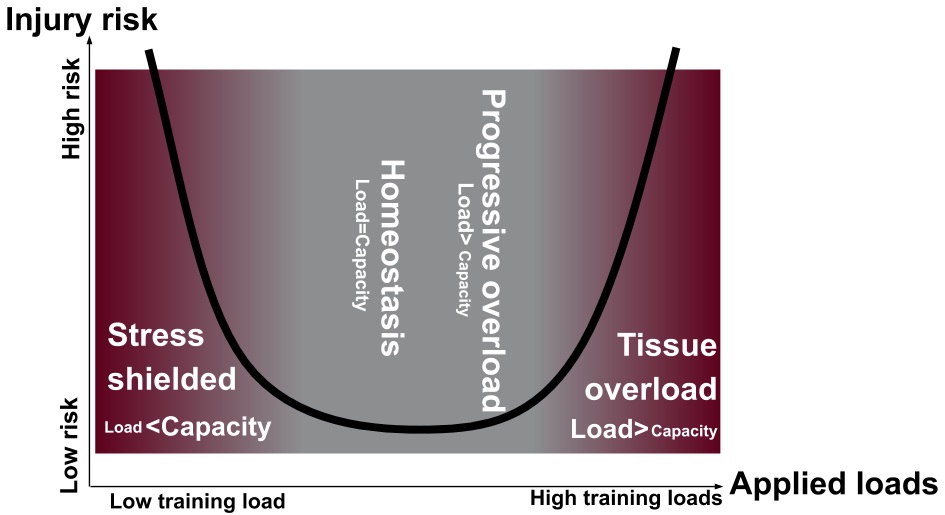
Figure 1: Tissue homeostasis model, as per Dye 2005 and recently updated by Gabbett 2016.
Key points: A) The runner will not be able to return to running without progressive overload to restore the envelope of function; B) Stress shielding the injured runner will increase the risk of re-injury as much as tissue overload.
Overall strategy for rehabilitation of the runner with ITB pain
Well-designed rehabilitation programs for ITB pain aim to progressively overload the injured runner and the ITB to restore tolerance running-specific loads, also known as the envelope of function (Figure 1).(6,11) Using progressive overload, applied loads adequately challenge the system to stimulate adaptation, but the loads are not so excessive that the injured ITB is further irritated by extending into tissue overload.
Stress shielding, however, is as likely to cause re-injury as tissue overload because the runner will not be adequately prepared for the biomechanical loads that will be encountered during the return-to-run process.(12) As eluded to in part 1, clinicians and runners should both be careful not to fall into the stress shielding trap in an effort to reduce ITB pain.
Wait! Where does foam rolling fit into the tissue homeostasis model?
Foam rolling is often prescribed for ITB pain. However, foam rolling does not result in changes in flexibility that last more than just a few minutes(22) and any pain relief experienced by foam rolling is temporary, likely due to temporary central pain modulation.(1) Contrary to popular opinion, “adhesions” or “myofascia” are not being “released” or “broken up” by foam rolling.(3) Considering ITB pain is a compression injury(8), it makes little sense to add further compression to the lateral knee anyway.
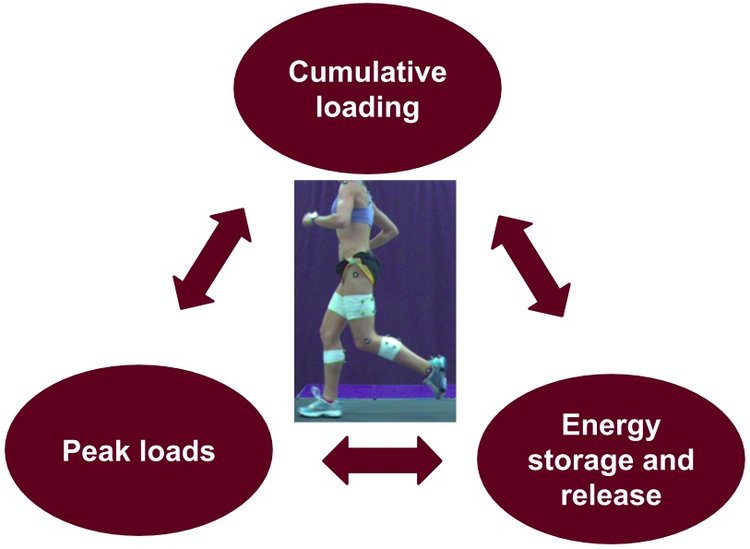
Figure 2: Three main components of loads experienced by the runner. Adapted from Willy & Meira 2016.
Instead of foam rolling, purposively target running-specific loads
During a typical run, anatomical structures experience a) high peak loads; b) with high levels of energy storage and release; c) in a highly cumulative manner (Figure 2).(26) All three of these components of loading should be addressed during rehabilitation: Peak loads are addressed with heavy, slow resistance training; energy storage and release demands are addressed with plyometric exercises; and, cumulative loading should be addressed by a graded return-to-run program (Figure 3).(26 )
Rehabilitation programs should carefully consider that the ITB is under load during running when hip adduction increases and step width narrows(14,18). The knee varus moment (outward bowing torque) increases as step width narrows, and also increases ITB load.(9,17) Finally, the ITB serves as a massive energy and storage release mechanism, particularly during terminal stance when hip extension is eccentrically coupled with knee flexion. We will leverage these aforementioned functions of the ITB to initially reduce irritability and then in the later stages of rehabilitation, restore capacity of the ITB.
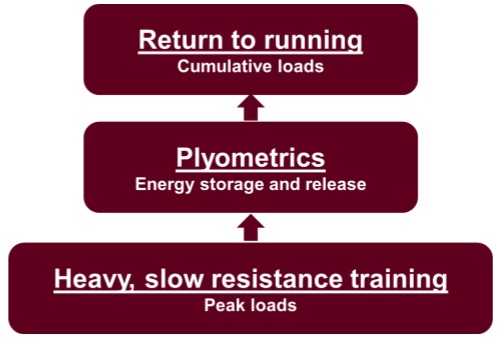
Figure 3: Addressing each component of loading is key to a successful rehab plan. Willy & Meira (2016) IJSPT.
Stages of rehabilitation for ITB pain
ITB pain rehabilitation is divided into two main phases; a) Pain Dominant phase and b) Load Dominant phase (Figure 3). These phases are derived from previous works of Cook and Purdam (2009)(4) (summarized superbly here by Tom Goom, PT) and Fredericson and Weir (2005).(10) Overall, these phases aim to maximize loading while keeping lateral knee irritation capped at 0-2/10 visual analog scale (VAS), either during the session or upon waking the next morning.
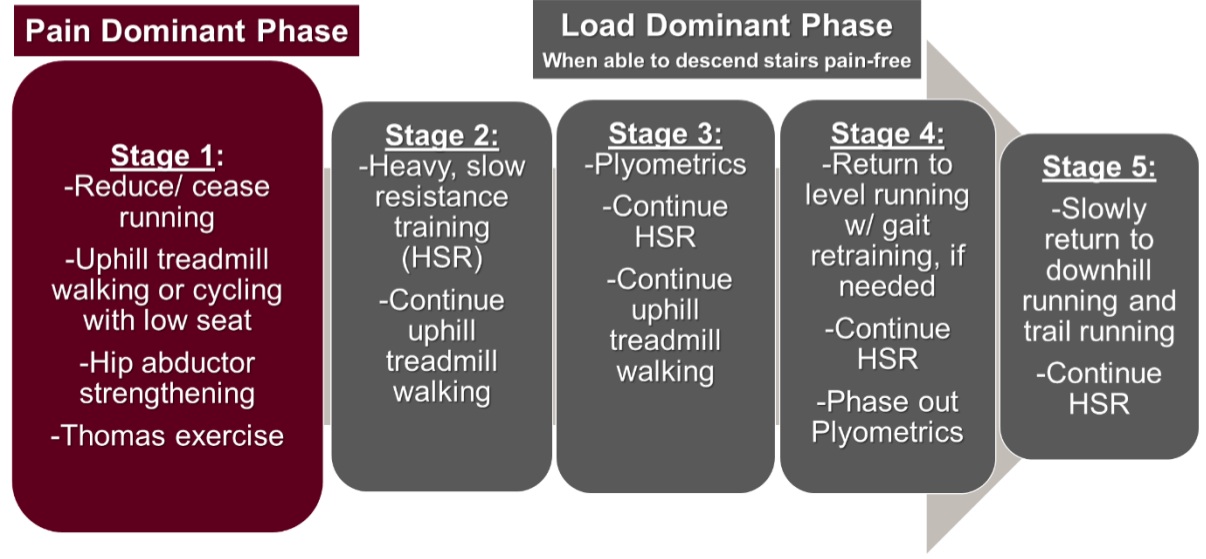
Figure 3: General progression of rehabilitation for the runner with ITB pain
Pain Dominant Phase: Decrease irritation without sacrificing too much capacity
Stage 1:
Load management is critical during Stage 1 to reduce irritation. Step descent and even fast walking is often painful in the Pain Dominant phase, resulting in cessation of running. The challenge is to reduce abusive loads and irritation of the ITB while maintaining loading as tolerated. Overall, loading improves tissue qualities16 while playing an important role in altering pain processing (Please see here for an excellent review).(21) Thus, activity levels should still remain as high as possible and we should not shy away from loading the ITB but without further exacerbating ITB pain. As a result, running may need to temporarily cease and be replaced with challenging, yet non-irritating activities.
During Stage 1, activity levels can be relatively maintained via vigorous uphill treadmill walking at an 8-10% grade. Uphill treadmill walking a)reduces the knee varus moment while increasing knee flexion at footstrike(13) to avoid the ITB impingement zone (~30 deg knee flexion)(7); and, b) reduces energy storage and release demands of the ITB. The treadmill is great because there is no need to walk downhill which is associated with high knee varus loads and high ITB energy storage and release demands
If uphill treadmill walking is not initially tolerated, stationary cycling is a good option. However, the seat should be moved forward and lowered slightly such that knee is flexed about 35 degrees at the bottom of the pedal stroke to keep the knee out of the impingement zone. If cycling is not tolerated, then swimming is a good option. However, the runner should always be working toward uphill treadmill walking, even if it is not tolerated initially.
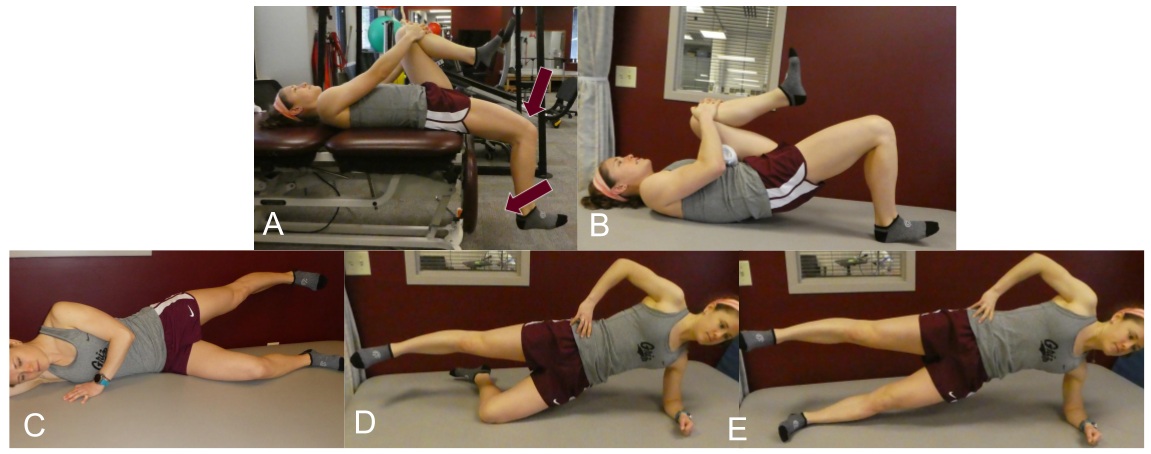
Figure 4: Stage 1 exercises. A) ITB excursion exercise (10×10” holds) progressing to (B) single leg bridge. Simultaneously, the runner is progressed through hip abductor progression (C-E).
Non-weight bearing, progressive ITB and hip loading exercises are initiated in Stage 1. The ITB is loaded throughout Stage 1 via the Thomas exercise, which is really just the Thomas test used as a low-load ITB excursion exercise (Figure 4A). The Thomas exercise is then progressed to a single leg bridge (Figure 4B). Concurrent with the Thomas and single leg bridge exercises, the posterolateral hip musculature are progressively loaded (Figure 4 C-E).(20) Multiple sets of isometric holds of 10 or fewer repetitions should be prescribed with adequate hold times and efforts that achieve near-muscular failure on the last couple of repetitions.
Load Dominant Phase: Stages 2-5
The runner transitions to the Load Dominant phase when s/he is able to descend stairs without pain.
Stage 2:
The split squat progression (Figure 5) is the cornerstone of Stage 2. This exercise progression eccentrically and concentrically loads the relevant musculature and ITB with heavy, slow resistance training via 6-second repetitions. The split squat essentially combines the ITB excursion exercises and isolated hip strengthening of Stage 2 into a single exercise. It should be noted that strengthening alone will not address any running biomechanics that are thought to contribute to ITB pain in the runner;(25) instead, strengthening exercises should only be viewed as loading exercises that will enhance load tolerance of the targeted structures. In other words, err on the side of more load rather than “functional.”

Figure 5: Split-squat progression. Key Point: the trailing (right) leg is the injured leg. The runner shifts as much body weight as possible through the right foot to load the right hip flexors while eccentrically lowering and concentrically raising the body. Repetitions are performed slowly (3 seconds descent, 3 second raise). Once the set is completed, the right leg is then switched to the front and weight is shifted to it to target the hip extensors. Initially, the table is set at a low height (A), then progressed to a raised position (B), followed by added resistance in C and D.
A typical progression might be 3 sets of 10-12 repetitions unweighted split squats, eventually progressing to 4 sets of 6-8 repetitions with added weight, with near-muscular failure on the last repetitions. In Stage 2, the split squat is performed 3x/week with uphill treadmill walking continuing 3-7x/week. The split squat progression is done throughout Stages 2-5, with resistance progressed appropriately.

Figure 6: Resisted lateral skaters
Stage 3:
Plyometrics are added in Stage 3 in continued into Stage 4 to address the energy storage and release demands of the ITB but without the cumulative loading of running. This stage is short, generally just 1 week, and is used merely as a bridge between Stage 2 and Stage 4, where running is re-initiated. Resisted lateral skaters (Figure 6) are an excellent plyometric exercise due to the loads applied to the posterolateral hip musculature.
Stage 4:
An accelerated return to running program is often be used after completing stages 1-3 to reintroduce running loads in a graded manner. Please see here for a free download. It is critical for the runner to view the return to running program as merely another form of “loading exercise.” If the runner views running as a means to gain fitness, the runner will often break from the return to run process and do too much running too soon. Use challenging crosstraining e.g., stationary cycling intervals, to maintain aerobic fitness during the return to run process.
Many runners with ITB pain benefit from completing the initial 2 weeks of return to running with a moderate grade (5%) on a treadmill prior to transitioning outside. Downhill and trail running (results in narrow step width) should absolutely be avoided at this stage. Patient education is crucial here as the runner is anxious to return to a full training load and may repeat the same training mistake that resulted in the initial bout of ITB pain. Plyometrics from Stage 3 are phased out in the second or third week. Gait retraining is an excellent adjunct to reduce loads during running to allow longer running prior to the onset of symptoms. The simplest, and perhaps most effective, retraining technique to is cue a 5-10% increase in running cadence which a) reduces peak hip adduction(15,24); b) increases step width(2); c) results in a more flexed knee at footstrike(23) thus minimizing time in the ITB impingement zone. Most importantly, adopting a higher cadence reduces ITB strain and strain rate.(2)
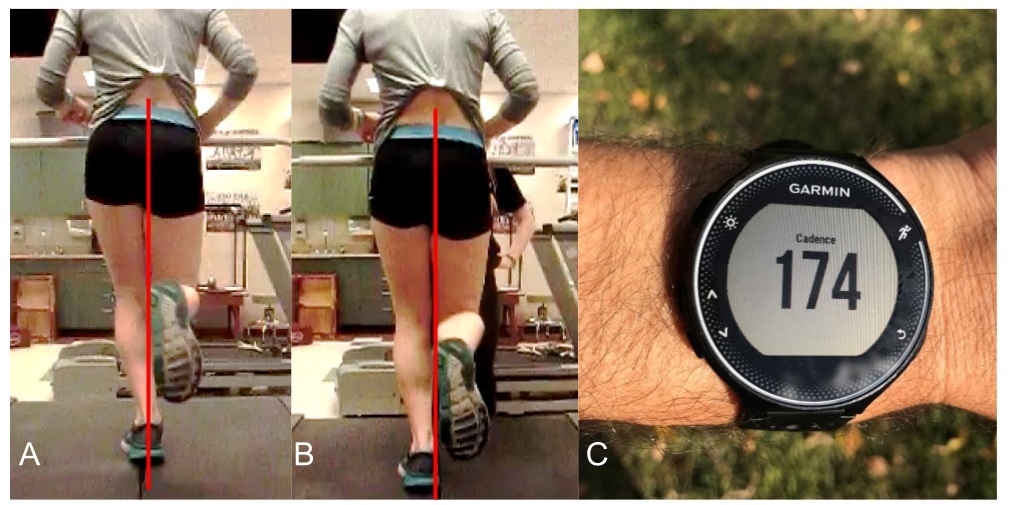
Figure 7: Runner with left ITB pain at baseline (A) and with (B) a 7.5% increase in running cadence over her preferred. Note the reduced crossover, reduced hip adduction, and pelvic drop in midstance. Feedback on cadence was provided with a Garmin GPS running watch (C).
Merely cueing a runner to increase their cadence is not sufficient; any retraining intervention must have a feedback component so that the runner can detect their errors and sufficient practice in order to be effective.(5) Most runners use GPS watches that can also provide feedback on running cadence (Figure 7).
Other gait modifications may be indicated, such as directly cueing a reduction in hip adduction(19,27) or cueing an increase in step width(18).
Key point: gait modifications should address running biomechanics that are specific to the runner you are treating.
Stage 5:
In this stage, the runner should continue to increase training volume in a reasonable manner. Downhill running and trail running are gradually added, if applicable to the runner. However, the runner should add trail running and downhill running on separate days initially, prior to adding them together in a single run. Finally, the runner would benefit from continuing the heavy slow resistance training with the split squats, but should drop back to doing it just once a week as running volume increases.
Concluding thoughts
Considering the high demands runners place on the ITB, adopting an active rehabilitation approach for ITB pain seems warranted. While reducing loads makes sense in the pain dominant stage, it is critical for the runner and clinician to work toward restoring the full capacity of the ITB and the runner through a progressive overload approach.
This was originally posted on Rich Willy’s website. You can click here to read more blogs from him.
Want to learn more from Rich Willy?
He has done a Masterclass lecture series for us on:
“Restoring load capacity in the injured runner”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!