Iliotibial Band Pain in the Runner Part 1: Etiology and Assessment

This is the first of two-part series by Rich Willy, PT, PhD, on Iliotibial band (ITB) pain. ITB pain is a common injury in runners, but there is little guidance in the literature for treating this tricky injury. This series aims to shed some light on the etiology (Part 1) and treatment (Part 2) of this often frustrating injury.
What is Iliotibial band pain and who gets it?
Iliotibial band (ITB) pain is the primary source of lateral knee pain in runners, representing between 5% and 14% of running-related injuries.(14) ITB pain is more commonly experienced by male runners (50-81% of runners with ITB pain) versus female runners.(14) Pain is localized over the lateral femoral condyle as the knee flexes and extends over an arc of 25-35 degrees of knee flexion, classically known as the impingement zone.(10) Knee pain is reproduced as the hip extends while the knee flexes as the tensor fascia latae musculature is loaded eccentrically,(1) such as during downhill running or stair descent. Runners with acute ITB pain describe a pain quality that is sharp, requiring cessation of running.
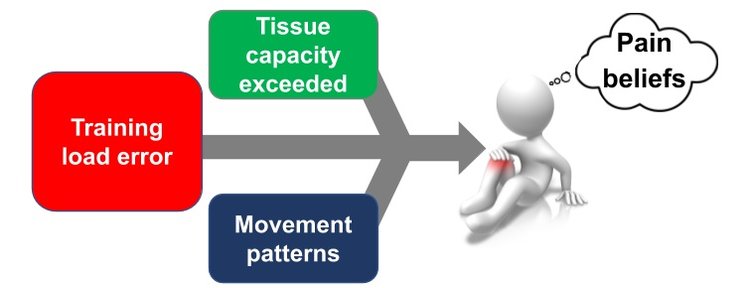
Figure 1: Factors relating to etiology and recovery from ITB pain
All Running Injuries are training load injuries. (5) ITB Pain is no exception
Runners who rapidly increase running volume(8), particularly downhill,(10) are at risk for ITB pain. Running with a narrow step width(7) (as during running on a narrow trail) or running with higher amounts of hip adduction(4,9) increase strain in the ITB (See Figure 2 below). Most importantly, a runner can have the aforementioned running biomechanics and relatively low tissue capacity, but an injury will not occur without a rapid, relative increase in applied training loads. Once injured, the runner’s load capacity will reduce substantially and pain will then be experienced during even relatively benign activities, such as step descent.
While not studied directly in runners with ITB pain, the presence of fear avoidance beliefs is a strong predictor of slow recovery from other non-traumatic knee pathologies, such as patellofemoral pain.(11)
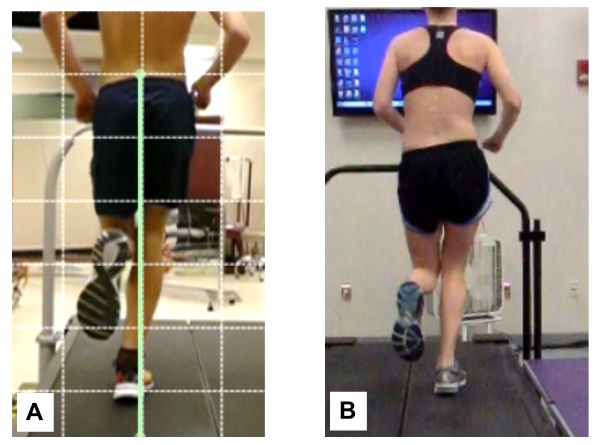
Figure 2: Runner A demonstrates a narrow step width pattern and Runner B demonstrates a high hip adduction running pattern. Both increase strain in the ITB
ITB pain can quickly become a persistent injury
Runners will often temporarily cease running when ITB pain occurs, causing the irritability to decrease. However, because the runner is avoiding loading the ITB (also known as stress shielding), the ITB and the runner unknowingly lose even more load capacity. The runner is then fooled into thinking that their injury is better. Since the runner is keen to return to running, an activity that they love, the return to run process is rushed. The runner essentially repeats the same training error that initially caused their injury. This process is repeated, resulting in continued loss of load capacity (Figure 3).
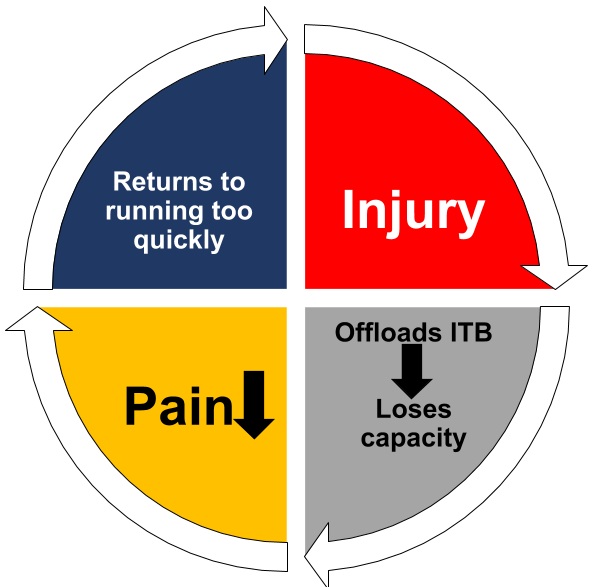
Figure 3: Cycle of loss of load capacity
ITB pain is a compression injury. So, let’s stop calling it a “friction syndrome.”
The ITB is really just a thickening of the lateral thigh fascia and has considerable attachments to the femur and patella, prior to attaching distally to the Gerdy’s tubercle (cadaver knee figure).(2) The consistent tethering of the ITB to the lateral femoral condyle and supracondylar ridge effectively prevents the ITB from flipping over the lateral epicondyle. In other words, no friction here.(3)
In the runner with ITB pain, the highly innervated adipose tissues that lie between the ITB and the lateral femoral condyle are compressed as the knee flexes past 30 degrees as peak tension is reached in the ITB (cadaver video). This compression is nociceptive and has potential to be painful.(2,3)
There is no single good test to diagnose ITB Pain
ITB pain is diagnosed based on patient history i.e, recent relative increase in overall running volume and downhill running, but it is also a diagnosis of exclusion. Other sources of lateral knee pain should be excluded including patellofemoral pain, gluteal tendinopathy, lumbar spine referral, and distal femoral stress fracture. Imaging is typically only done to rule out other pathologies and is not particularly diagnostic for ITB pain.(6)
The Noble compression test or the modified Noble compression test is suggested to enhance probability of accurate diagnosis of ITB pain. The modified Noble compression test (Figure 4) places the hip in extension as the examiner passively extends an internally rotated knee while compressing 1-2 cm proximal to the lateral femoral condyle to assess for the presence of pain.(13) The positive and negative likelihood ratios are unknown for either version of the Noble compression tests, so tread lightly when using them. In other words, rely on patient history while ruling out other possible sources of pain.

Figure 4: Modified Nobel Compression test
The OBER test is a terrible test for ITB “tightness”. It’s time to stop doing it.
In a recent cadaver study, the Ober test, either the classic or the modified versions, was not affected after the ITB was transected, i.e., cut.(15) The largest contributor to a “positive” Ober test was the hip capsule followed by the gluteus medius and minimus musculature.(15) Even if the ITB was “tight”, it’s physiologically impossible to stretch it.
It’s all about hip weakness, right? Um, not really.
Hip weakness is not a predictor of who will develop ITB pain, yet individuals with ITB pain have hip weakness.(14) This suggests that ITB pain causes hip weakness rather than the other way around, similar to what has been proposed in patellofemoral pain.(12) Intriguingly, Fairclough and colleagues postulated that compression of the highly innervated soft tissue between the ITB and the lateral femoral condyle results in inhibition of the proximal musculature, resulting in a maladaptive strategy to reduce compressive forces acting on the tissue beneath the ITB.(3) Still, hip strengthening seems to be an important component of rehabilitation for ITB pain, as we will discuss in Part 2 of this blog series.
In part 2 of this blog series, we will discuss treatment progressions and return to run recommendations for the runner with ITB pain.
Want to learn more from Rich Willy?
He has done a Masterclass lecture series for us on:
“Restoring load capacity in the injured runner”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Leave a comment (1)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Nice and helpful article for every runner who suffering from ITB pain. ITB pain is more commonly experienced by male runners. So Never ignore take the best sports physiotherapy for injuries.