6 Tips to Improve your Isometric Exercise Prescription

So you’ve been using isometric exercises in your rehabilitation practice for a while, right? Surely there’s not much to them?
You already know they are a great entry point for lots of resistance training applications. They are easy to teach, almost anyone can do them, and you’ve even read that paper by Ebony Rio et al about how doing a hard wall sit for about 45 seconds can decrease pain in patellar tendinopathy (1).
Step 1: Sit against the wall
Step 2: Hold it for a while until you get tired
Step 3: Hope it gives some pain relief
Well hopefully this article can open up a whole new world of possibilities for your isometric exercise prescription in rehabilitation and performance capacity. Before we get into it, If you want to learn more about exercise prescription, check out this masterclass by Dr. Teddy Willsey.
The following 6 tips will be your guide to getting the most out of your isometric exercise prescription.
Tip 1
There is more than just 1 type of isometric exercise. In fact, you intuitively already know the main 2 as we use them every day.
1. Hold (yielding) type:
- Sustaining a set joint position under a constant external load for a set amount of time.
- The load is acting to try to change the joint position – aka it is attempting to perform “negative work” on the system
- If the load is too much we get a eccentric lowering / yielding of the load / bodyweight
- Eg a wall sit (see below video)
2. Push (overcoming) type:
- Sustaining a set joint position while attempting to move an immovable object
- The external load doesn’t attempt to create any negative work on the system. Instead the muscular force is attempting to create “positive work” into the system
- If the force output is too great for the object we get an “overcoming” of the object we were pushing on and therefore a concentric contraction.
- Eg an isometric deadlift (see below video)
When compared for the same intensity of contraction, a hold type will fatigue and fail at a quicker rate than a push type (2).
Within these subtypes we have 3 main contraction velocities:
- Sustained: Here the goal is to maintain the same force output throughout the whole rep.
- Main uses are pain modulation, endurance and hypertroph
- Ramped: Here the goal is to gradually increase force output over the rep
- Main uses are hypertrophy and strength gains
- Ballistic: Here the goal is to rapidly produce a maximal force for a rep of very short duration
- Main uses are increasing rate of force development (RFD), power and strength adaptations (3-5).
Tip 2
Isometric training doesn’t mean less gains.
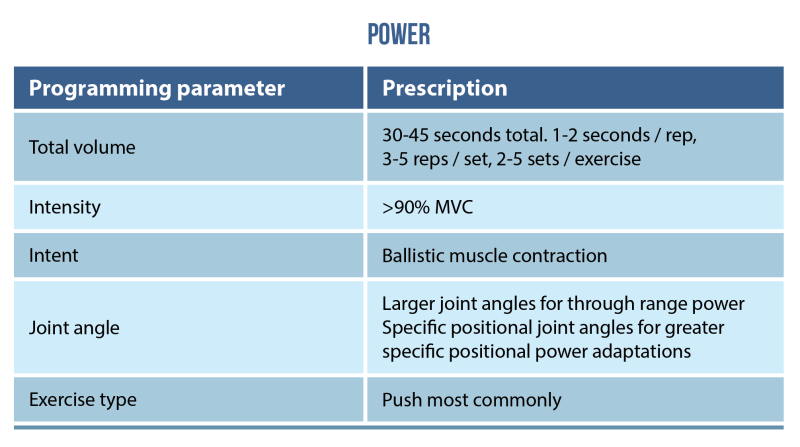
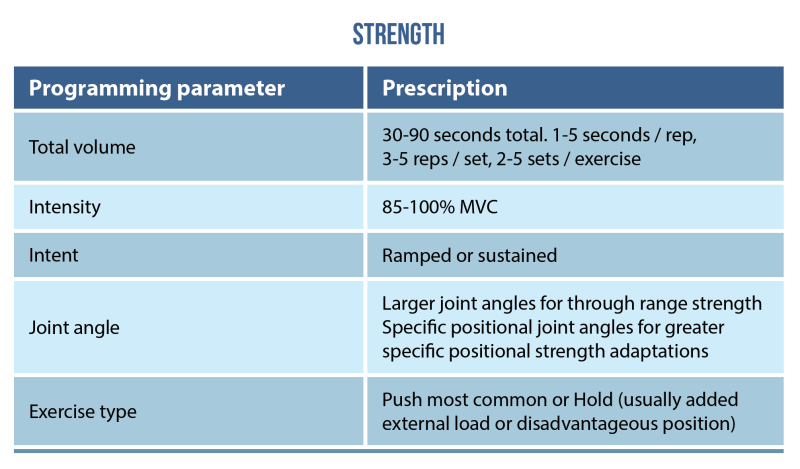
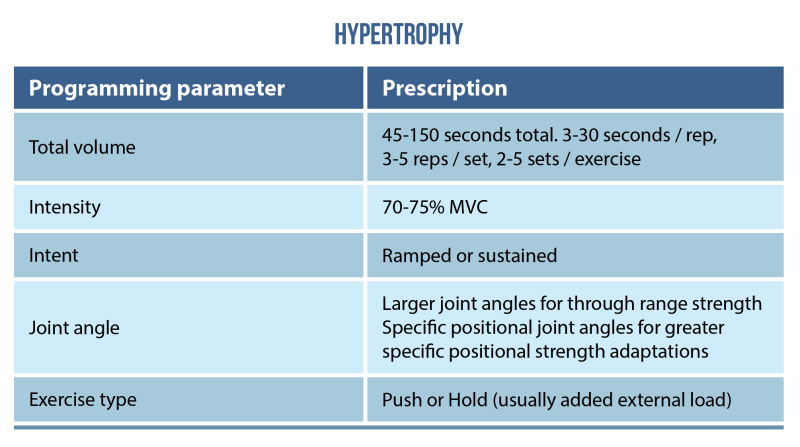
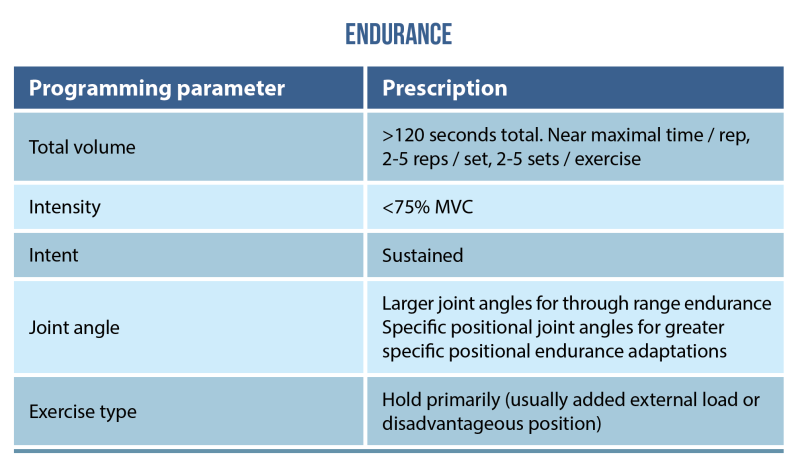
Evidence now suggests that the following modifiable variables will allow you to select for multiple morphological and neurological adaptations:
- Total volume (TUT): sets X reps X time/ rep
- Intensity of contraction: % Maximum Voluntary Contraction (MVC)
- Intent: rate of force development (RFD)
- Joint angle: large or small
- Exercise sub type: push or pull
Here are the pragmatic programming recommendations for specific purposes (4,5).
Tip 3
Like in my previous blog on cluster sets, isometric training protocols are a great way to minimize the fatigue generated from a bout of training stimulus (4-7).
However, the way we achieve this is very different, and hence isometric training can be another useful tool when the stimulus : fatigue relationship is important (5,7). Due to the lack of any change in muscle length under contraction, isometric training in general creates less muscle damage and therefore recovery burden (7-10). In contrast to tools like cluster sets, the acute metabolic response from isometric training is usually quite high (think the burn you feel in a wall sit / plank).
Tip 4
Unique stimulus for tendon adaptation.
Isometric exercise, like most others, when programmed appropriately will see positive physiological and performance adaptations for the tendon. In general, what is occurring during adaptation to repeated isometric training stimuli, is that the tendon’s mechanical properties (young’s modulus) and hence material property (stiffness) is changing greater than morphological ones (CSA, composition etc). This differs from regular isotonic resistance training which also tends to promote a greater increase in CSA (11,12).
Isometric training has even been proposed to have a more efficient stimuli : adaptation relationship than plyometric training in regards to increasing tendon stiffness. This is because during plyometric type training the peak forces are so high, but durations so short that much of the energy is lost in hysteresis and therefore not utilized as productively for mechanotransduction (5,11). The sustained contraction type means that isometrics can be an easily controlled stimuli for adaptation.
The best dosage for tendon adaptation sits within the strength training type prescription outlined above (5,11).
Tip 5
Isometrics are safe and well tolerated.
Isometric muscle training has often been cautioned against in many of our special populations due to fears of cardiovascular complications resulting from high blood pressure (13). Many of the research protocols identify participants reaching high systolic blood pressures and increases in heart rate (13-15). These protocols often cite a 25% below baseline supercompensation effect that occurs in the minutes after the testing for both measures (14,15). However, when you investigate these further, we see a relationship between cardiac response and isometric contraction that is mediated by:
- Length of time per contraction
- Number of consecutive reps of isometric holds with minimal rest.
- Greater muscle mass used (14,15)
Therefore, from a safety perspective, isolation exercises of shorter duration holds with intraset rests would be best if safety was a concern (eg cluster set).
Tip 6
Useful for pain modulation.
Now this is a weird one. As the current state of the literature would suggest, there is no one silver bullet here for pain modulation. What seems to work for the patella tendon (eg 5 x 45 sec @ 70%MVC) (1,16), doesn’t work for the achilles (17), or lateral epicondylalgia (18). However, what we do know from general pain physiology studies can give us some starting points to work from and adapt accordingly to our clients response (19-21).
- There appears to be a intensity threshold (around 25% MVC and above)
- There appears to be a proximity to failure threshold (around a sustained 10% drop in MVC from peak across a rep)
- There appears to be a relationship between required TUT and intensity of contraction, where more intense contractions require less total time to elicit significant pain modulation.
Due to this heterogeneity in the pain modulatory response, I would advise using isometric training the following way with painful conditions:
- Find a pain free / pain tolerable position to train the injured site in
- Select a suitable biomotor training prescription as outlined above based on the goals of the intervention
- Apply the lowest required dose to get the desired response that meets the biomotor prescriptions as well as our general principles above
- Check response and adapt as required. (eg they didn’t tolerate the intensity of a strength training prescription, move to more a hypertrophy type instead)
Wrapping up
So there you have it. Hopefully you have broadened your horizons and can start to really diversify your use of isometric strength training in the clinic. If you want to learn more about exercise prescription, check out this masterclass by Dr. Teddy Willsey.
Want to learn more about sports rehab?
Dr Teddy Willsey has done a Masterclass lecture series for us on:
“Exercise Prescription in Sports Rehab”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!