Rethinking the Posterior Talar Mobilisation and Mulligan Mobilisation With Movement (MWM)

The posterior talus mobilisation is by far one of the most utilised by practitioners, and the most popular self-mobilisation seen on social media at the foot and ankle. I stopped counting after seeing over 107 videos on Youtube of the popular banded self-mobilisation version seen in Figure 1. This mobilisation is particularly popular in part due to the fascination of “ankle” dorsiflexion and its often misunderstood importance in gait, various squat shapes, and sport movements. Limited ankle dorsiflexion has become a stereotypical presentation seen in several NBA players, in fact, due to the high occurrence of foot and ankle injuries it is often seen as a critical quality that practitioners across the league have fixated on improving. When I was introduced to the posterior talar mobilisation I saw a lot of practitioners utilising it, and it was one of the few mobilisations taught to improve ankle dorsiflexion in most manual therapy courses. After using it session after session with little to no chronic change with my NBA basketball athletes, I began to question its utility. Maybe you have had similar experiences as well?
The purpose of this article is to highlight the importance of the triplanar nature of the talocrural joint and its coupled relationships between the talocalcaneal (subtalar) joint, the talocalcaneonavicular joint, and the Chopart joint, to transition our thinking from simple to more complex. Through the lens of complexity, you will see that we have far more opportunity to assess and intervene at these joints than what is typically taught or understood.

The history of the Mulligan Mobilisation!
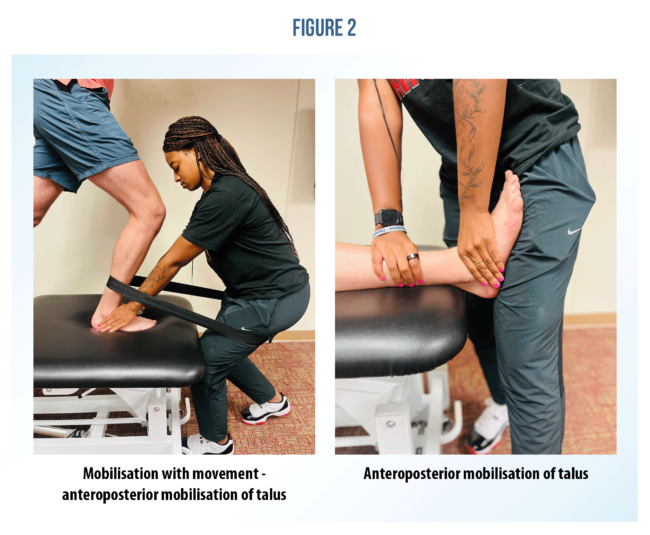
Most practitioners still utilise this mobilisation (Figure 2) popularised by Mulligan in 1999, but over time it is now being used differently than what was proposed 25 years ago. Collins et al. 2004 describes the mobilisation’s true intentions – “The Mobilisation With Movement (MWM) treatment approach for improving dorsiflexion post-lateral ankle sprain combines a relative posteroanterior glide of the tibia on talus (or a relative anteroposterior glide of the talus on the tibia) with active dorsiflexion movements, preferentially in weight-bearing (Mulligan, 1999)”.
This is the issue – the mobilisation was created to reduce the excessive anterior translation of the talus following an Anterior Talo-Fibular Ligament (ATFL), or lateral ankle sprain. Every article I came across from that period researched the use of that mobilisation with acute/subacute ankle sprains. Now practitioners simply use it to increase dorsiflexion because it matches the convex on concave arthrokinematics of the talocrural joint in open-chain dorsiflexion of the talocrural joint.
Convex-concave rules for closed chain-dorsiflexion of the talocrural joint, (tibia rolls and glides anteriorly on talus) do not support the use of a posterior glide. One may argue that providing a posterior stabilising force to the talus will facilitate the necessary relative motion to allow the tibia to rotate anteriorly more efficiently. That would make sense if this joint were purely a sagittal plane hinge joint. On the contrary, I would strongly advise against this method because it inhibits the conjunct rotation mechanism that accomplishes this very task that allows relative motion in the transverse (internal/external rotation) and frontal plane (eversion/inversion) between the talus and the tibiofibular complex, and the simultaneous coupled relationships between the talus and the talocalcaneal (subtalar), talocalcaneonavicular, and Chopart joints.
Biomechanics of heel strike and flat foot
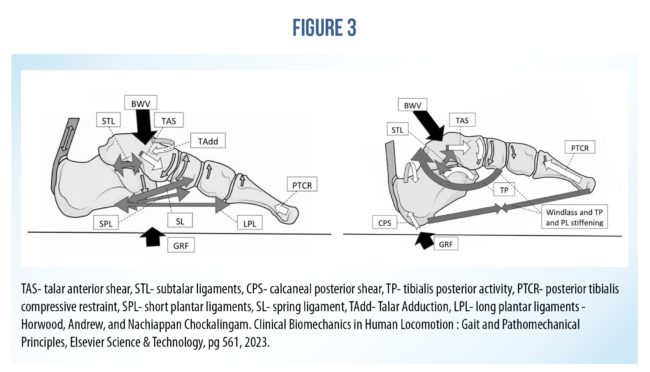
In asymptomatic patients, the talus never moves posteriorly during this process at all, in fact, as the posterior Ground Reaction Force (GRF) causes the heel to plantarflex, abduct, and slightly evert at heel strike during gait, the body weight vector moving anteroinferior translates down through the tibiotalar complex causing the talus to plantarflex, translate anteriorly, and adduct relative to the calcaneus, but abduct relative to the tibia! This anterior translation is resisted passively by the posterior talocalcaneal ligaments, interosseous ligament, and medially restrained via the cervical ligament. This motion is resisted actively by the posterior tibialis tendon (PTCR – see Figure 3) via a posterior vector that pulls the articular surface of the navicular into the head of the talus causing a compressive force closure of the talonavicular joint. Medially the talus is also resisted by the medial-inferior wall of the spring ligament of the talocalcaneonavicular joint (yes this is a real joint) and medial-lateral compression via the posterior tibialis and flexor digitorum longus tendons.
What is relative rotation and why is it so important?
In general, this topic can be very confusing due to a lack of consistent terminology and reductionist explanations to keep things simple, so a re-read may be in order. The goal of this explanation is to keep things simple without losing any high-yield details that are clinically relevant to your practice. The most important aspect to remember is that clear reference points must always be defined, or ambiguity may lead to misinterpretation.
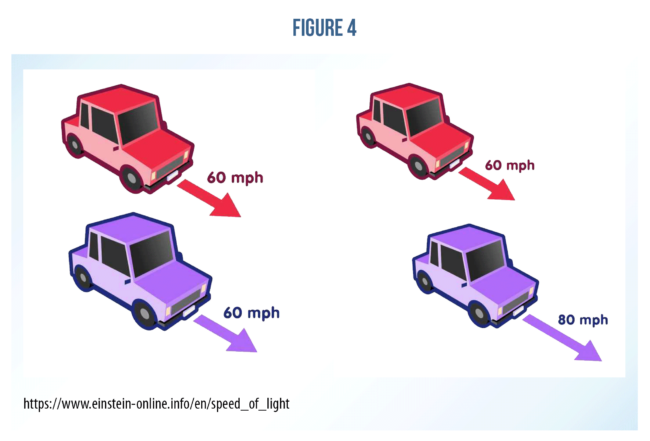
Relative rotation in this context is when two bones are articulating with one another and moving in the same direction, while one of those bones is moving slower than the other. You may have read that during “pronation” the talus is adducting during stance phases in gait. This is true, and also unspecified to mean talar adduction relative to the calcaneus. You see, without a reference point, these terms mean nothing and cause confusion. The easiest way to think about this is the old relative velocity example of two cars moving in the same direction from secondary school. In the first example, both cars are moving in the same direction at the same speed, therefore, from both car’s perspective, neither of them will appear to be moving (no relative motion). In the second example, the purple car is moving faster than the red car, so from the perspective of the purple car, the red car is moving backward and vice versa from the perspective of the red car, where the purple car seems to be moving forward (increase in relative motion).
The same can be said of the talus, tibiofibular complex, and the calcaneus. Simply put, until around “flat foot,” the talocrural joint is moving in opposite directions of the calcaneus in the vertical axis (adduction/abduction). During that same motion, the talus and tibiofibular complex are moving in the same direction but at different speeds, which allows for increased degrees of freedom within the talocrural joint. This relative rotation within the talocrural joint is key for proper dorsiflexion across the entire foot and ankle complex, and a posterior talar glide does not adequately address this.
Wrapping up
The purpose of mobilising joints is to give neurological input utilising proper biomechanics as the conduit to induce a desired adaptation over time. By performing this mobilisation chronically, I argue that we are at worst, driving anti-physiological input to the nervous system and local tissues that inhibit proper movement capacity, and at best just wasting our time.
Imagine a complex symphony performed by a full orchestra where each instrument plays a crucial role in producing harmonious music. Now, suppose there’s a section where two instruments seem slightly out of sync, which in turn changes the way the nearby sections play and propagates out even farther to the entire ensemble. If the conductor only focused on the initial section and adjusted the two instrument’s tempos that started the chaos, the initial issue between the two instruments might improve marginally, but the overall sound of the symphony would still underperform because the interconnected relationships between all the instruments have not been addressed.
The foot and ankle complex, akin to a beautiful symphony, is a biotensegrity complex that relies on the coordination of multiple degrees of freedom afforded by its 30 bones (I count sesamoids too), ligamentous structures, and musculotendinous units making it extremely dexterous. It is these relationships that make this complex so special and also difficult to teach and research. Nevertheless, we should strive to continue to study these complex interactions, as it is through these explorations that we may discover methods in which to reduce those persistent lower limb and foot injuries that continue to plague the NBA and many sports like it today.
Want to get better at treating ankle sprains?
Chris Bleakley has done a Masterclass lecture series for us on:
“Ankle sprain: etiology, diagnosis and rehabilitation”
Try it for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!