Mastering shoulder instability: Your management manual

Shoulder instability management can be challenging for physios – no one wants to have a patient dislocate their shoulder when returning to play. While we cannot eliminate the possibility of injury, we can build resilient shoulders that can handle the impact and load demands of the given sporting environment. In this blog, I’ll outline Hamish Macauley’s approach to the management of shoulder instability – if you’d like an in-depth understanding of how the experts manage shoulder instability, watch Hamish’s full Practical HERE.
My last blog outlined Hamish Macauley’s shoulder instability assessment Practical – using these tips, we will have determined a baseline of function and irritability, and we may have uncovered modifications that improve movement (e.g. cuing external rotator activation to improve overhead reaching). Following this assessment, we can then start with an exercise-based approach which includes:
- Strength and stability exercises
- Plyometric, reactive, and power training
- Return to sport drills
Note that there is massive variability in how patients respond to training, so we need options for modifying exercises on the fly. Below I have outlined where to start patients and what they should progress towards:
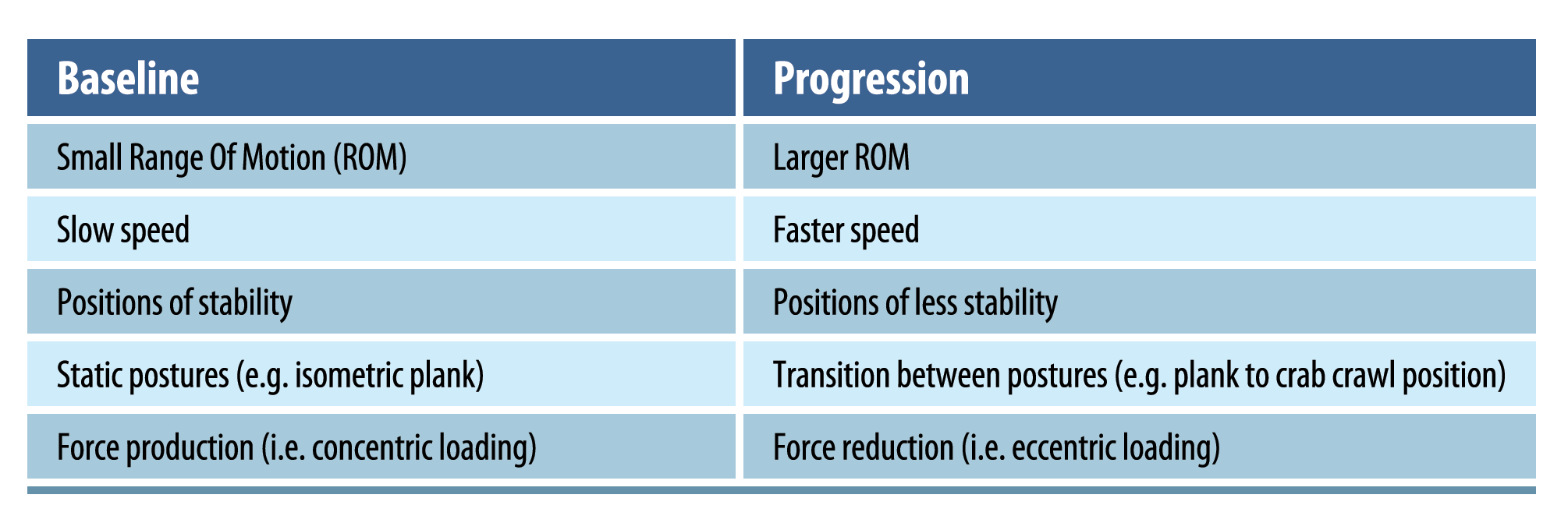
NOTE: Irritability must be accounted for when progressing an athlete. Minor pain during an exercise is ok, but it should mostly resolve by that night or the next day, before progressing them further.
Strength and stability exercises
A combination of Closed Kinetic Chain (CKC), Open Kinetic Chain (OKC), and isolated rotator cuff training should be used to rebuild shoulder stability. The sequence of positions for strengthening is:
- Horizontal loading (e.g. rows, quadruped)
- Vertical loading (e.g. pull down, downward dog)
- Outer range loading (e.g. “90/90” position, “Y” positions)
Closed Kinetic Chain Training
Typically, unstable shoulders respond well to CKC exercises, as the compression helps to stabilise the glenohumeral joint. An important caveat is that CKC positions are not the same for all types of shoulder instability. For example, with posterior instability, posteriorly directed forces on the shoulder (e.g. a plank position) can actually be higher risk and may need to be modified. On the other hand, with anterior instability, positions like shoulder extension may need to be introduced cautiously.
For most cases, a great starting point for CKC training is the quadruped position. Start with simply lifting one arm at a time, then lifting one leg, and then progressing to the bird-dog exercise. As the patient progresses, they can move towards crawling in multiple directions.
The intensity of the quadruped crawl can be increased by raising the knees, which adds substantially more load to the upper extremities. Next, the patient could progress to end-range positions such as a pike position and a crab walk. Note that transitions between postures are typically more challenging to the shoulder, which Hamish demonstrates in the video taken from his Practical below:
CKC training can also be progressed by adding perturbations from the therapist. This unique stimulus begins training the shoulder to react to unexpected, rapid loads, to meet the demands of the sporting environment.
Open kinetic chain training
These exercises are excellent for promoting rotator cuff activation, stabilising the shoulder at end ranges, and promoting healthy scapular movement.
Generally, it is useful to start with horizontal pressing and pulling (e.g. rows and chest presses). Then we can work into vertical pressing and pulling, such as pull downs and overhead presses. Note that when performing most of these OKC exercises (with the exception of the bench press), it is important to promote scapular movement (i.e. we should not be cueing scapular retraction the whole time!). The scapulae need to glide on the ribcage and we need to train stability at end ranges of motion to replicate sporting demands. As the patient masters these basic movements, they can progress into movement patterns that train the whole kinetic chain to work with the shoulder. Examples include a squat to row and standing press, see Hamish demonstrate this in the below snippet taken from his Practical:
Isolated rotator cuff training
The rotator cuff is active in every movement of the shoulder. When pressing, the external rotators are primarily activated to stabilise, while the internal rotators are the predominant stabilisers in pulling movements. With movements like scaption and abduction, all rotator cuff muscles should be working. Hamish reminds us that we may not need a high volume of isolated rotator cuff exercises, as OKC and CKC movements train the rotator cuff quite well. However, if a patient still demonstrates major strength deficits, isolated rotator cuff training can be helpful.
Plyometric, reactive, and power training
Plyometric and reactive training
When a patient can tolerate full ROM strength exercises, we can start introducing plyometric and reactive training. Start with safe positions, like underhand ball tosses against the wall. Then progress to ball bounces in flexion, then overhead positions and the “90/90” position. Here, the focus is not on power development, but rather training the shoulder’s ability to react to rapid loading.
In addition, it’s important to train the posterior rotator cuff with drop-and-catch drills. The patient can start from 90-degrees of flexion in standing and progress towards a “90/90” position in prone.
Plyometric training culminates in force reduction drills, which typically are performed after a baseline of strength and force production (power) are developed. These include drills like falling into a pushup and land-and-roll drills. Watch this video taken from Hamish’s Practical in which he demonstrates progressions for eccentric control drills:
Power training
This can start with OKC exercises performed at high speeds, such as landmine presses. We can also add in medicine ball slams, first in the sagittal plane, then slams to each side. Other power training drills include pressing patterns that build from previous drills (i.e. the standing press).
Return to sport drills
In terms of preparation for return to sport, we need to test the shoulders for adequate fitness and symmetry. These tests, like dynamometer manual muscle testing and the Y-Balance test are covered in full depth in Hamish’s assessment Practical.
Return to sport drills further add reactive demands and expose the shoulder to the movement patterns of the sport. Other examples of return to sport drills include palming and tackling drills (i.e. for rugby). At this point in rehab, there is a high variability in training because specific sport demands will dictate what drills an athlete needs.
Wrapping Up
Expert shoulder instability management includes training strength, plyometric capacity, and sport-specific movements in a variety of ways relevant to the patient’s needs. Also, we need to keep the variables of progression in mind, as this plays a big role in continuing to challenge patients while avoiding irritating the shoulder.
For a full, expert run-down on how to master your management of shoulder instability in athletes, check out Hamish’s full Practical HERE.
👩⚕️ Want an easier way to develop your assessment & treatment skills?
🙌 Our Practical video sessions are the perfect solution!
🎥 They allow you to see exactly how top experts assess and treat specific conditions.
💪 So you can become a better clinician, faster.

Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!